

Centralization of High-Risk Cancer Surgery Within Existing Hospital Systems
- PMID: 31251691
- PMCID: PMC7351344
- DOI: 10.1200/JCO.18.02035
Centralization of High-Risk Cancer Surgery Within Existing Hospital Systems
Abstract
Purpose: Centralization is often proposed as a strategy to improve the quality of certain high-risk health care services. We evaluated the extent to which existing hospital systems centralize high-risk cancer surgery and whether centralization is associated with short-term clinical outcomes.
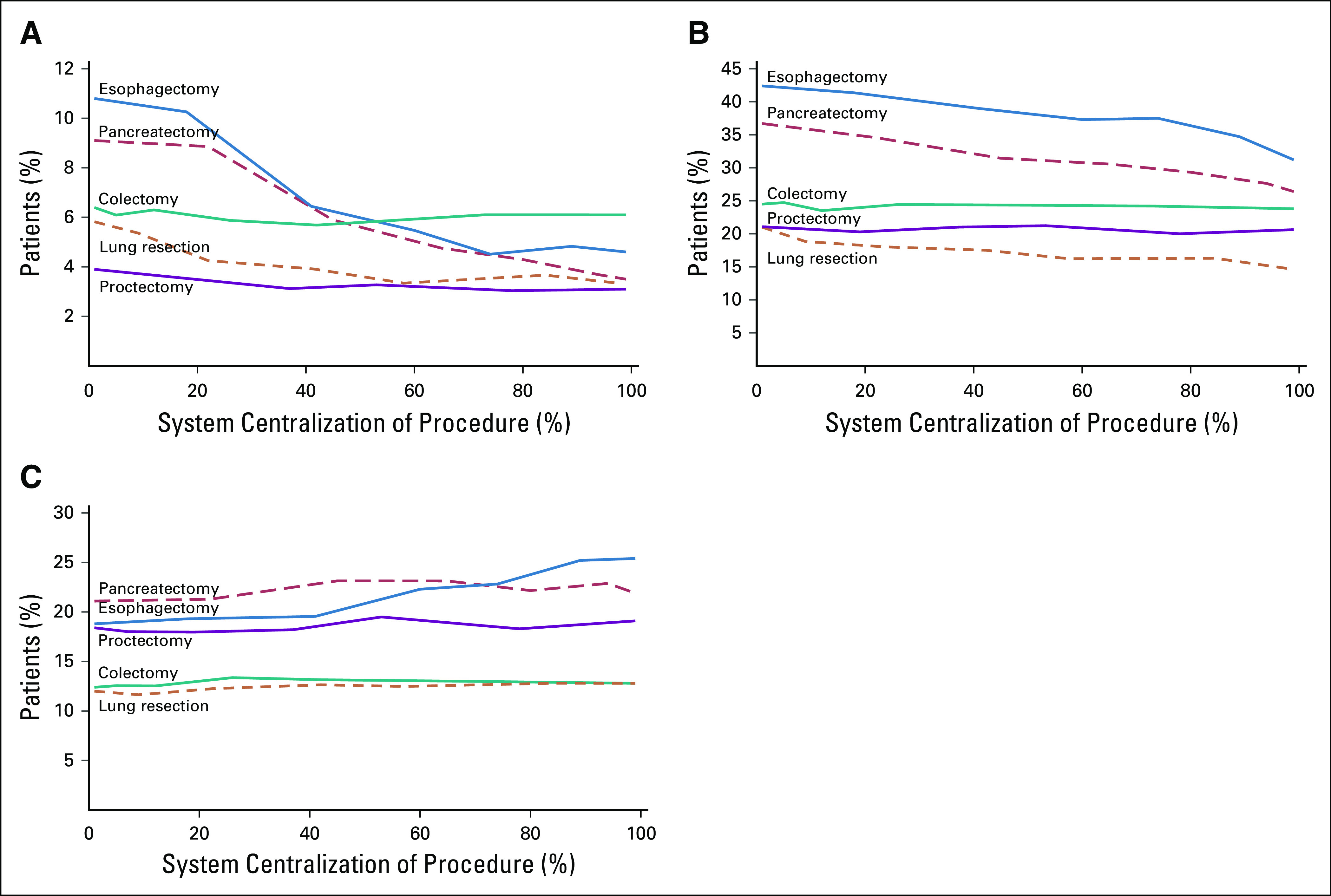
Patients and methods: We merged data from the American Hospital Association's annual survey on hospital system affiliation with Medicare claims to identify patients undergoing surgery for pancreatic, esophageal, colon, lung, or rectal cancer between 2005 and 2014. We calculated the degree to which systems centralized each procedure by calculating the annual proportion of surgeries performed at the highest-volume hospital within each system. We then estimated the independent effect of centralization on the incidence of postoperative complications, death, and readmissions after accounting for patient, hospital, and system characteristics.
Results: The average degree of centralization varied from 25.2% (range, 6.6% to 100%) for colectomy to 71.2% (range, 8.3% to 100%) for pancreatectomy. Greater centralization was associated with lower rates of postoperative complications and death for lung resection, esophagectomy, and pancreatectomy. For example, there was a 1.1% (95% CI, 0.8% to 1.4%) absolute reduction in 30-day mortality after pancreatectomy for each 20% increase in the degree of centralization within systems. Independent of volume and hospital quality, postoperative mortality for pancreatectomy was two times higher in the least centralized systems than in the most centralized systems (8.9% v 3.7%, P < .01). Centralization was not associated with better outcomes for colectomy or proctectomy.
Conclusion: Greater centralization of complex cancer surgery within existing hospital systems was associated with better outcomes. As hospitals affiliate in response to broader financial and organization pressures, these systems may also present unique opportunities to improve the quality of high-risk cancer care.
Figures
References
-
- Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized? The empirical relation between surgical volume and mortality. N Engl J Med. 1979;301:1364–1369. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–1137. - PubMed
-
- Birkmeyer JD, Stukel TA, Siewers AE, et al. Surgeon volume and operative mortality in the United States. N Engl J Med. 2003;349:2117–2127. - PubMed
-
- Urbach DR. Pledging to eliminate low-volume surgery. N Engl J Med. 2015;373:1388–1390. - PubMed
-
- Vonlanthen R, Lodge P, Barkun JS, et al. Toward a consensus on centralization in surgery. Ann Surg. 2018;268:712–724. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
