

Effects of dexamethasone on post-operative cognitive dysfunction and delirium in adults following general anaesthesia: a meta-analysis of randomised controlled trials
- PMID: 31253079
- PMCID: PMC6599229
- DOI: 10.1186/s12871-019-0783-x
Effects of dexamethasone on post-operative cognitive dysfunction and delirium in adults following general anaesthesia: a meta-analysis of randomised controlled trials
Abstract
Background: Several studies have investigated the effects of dexamethasone on post-operative cognitive dysfunction (POCD) or post-operative delirium (POD); however, their conclusions have been inconsistent. Thus, we conducted a meta-analysis to determine the effects of dexamethasone on POCD and POD in adults following general anaesthesia.
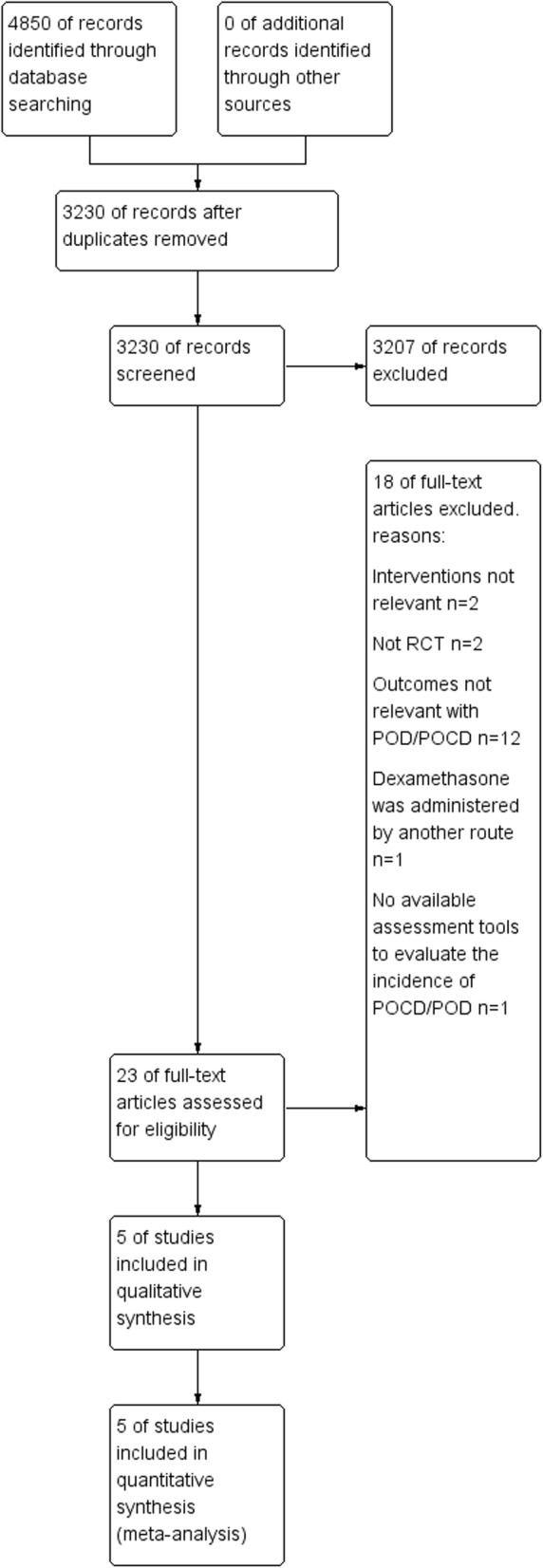
Methods: The Cochrane Central Register of Controlled Trials (2018, Issue 11 of 12) in the Cochrane Library (searched 17 November 2018), MEDLINE OvidSP (1946 to 16 November 2018) and Embase OvidSP (1974 to 16 November 2018) were searched for randomised controlled trials that evaluated the incidence of POCD and POD following dexamethasone administration in adults (age ≥ 18 years) under general anaesthesia. We used the Grading of Recommendations, Assessment, Development and Evaluations framework to assess the quality of the evidence.
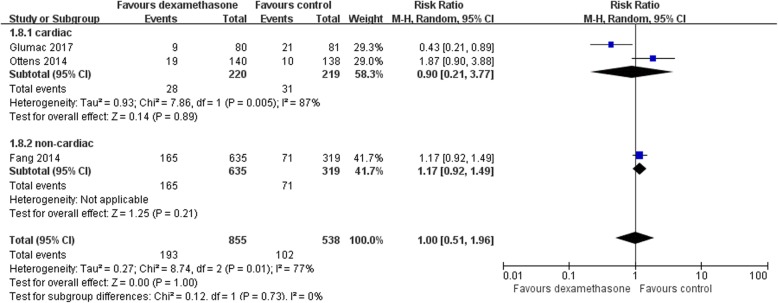
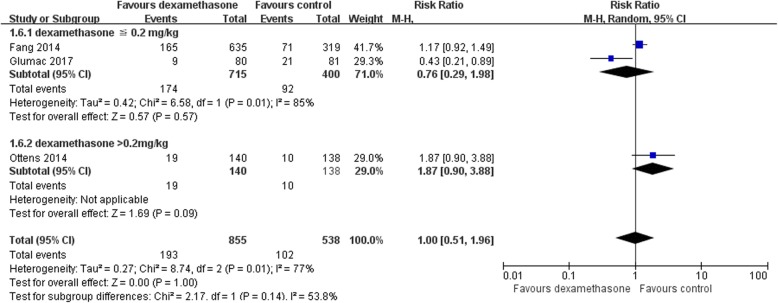
Results: Five studies were included (three studies with 855 participants in the dexamethasone group and 538 participants in the placebo group for the incidence of POCD, and two studies with 410 participants in the dexamethasone group and 420 participants in the placebo group for the incidence of POD). There was no significant difference between the dexamethasone group and the placebo group in terms of the incidence of POCD 30 days after surgery (RR [relative risk] 1.00; 95% CI [confidence interval: 0.51, 1.96], P = 1.00, I2 = 77%) or the incidence of POD (RR 0.96; 95% CI [0.68, 1.35], P = 0.80, I2 = 0%). However, both analyses had some limitations because of limited evidence and clinical heterogeneity, and we considered the quality of the evidence for the post-operative incidence of POCD and POD to be very low.
Conclusions: This meta-analysis revealed that prophylactic dexamethasone did not reduce the incidence of POCD and POD. Trials of alternative preventive strategies for POCD and POD, as well as a better understanding of the pathophysiology of those complex syndromes, are still needed to make progress in this field.
Trial registrationr: This study is registered with PROSPERO, 23 October 2018, number CRD42018114552. Available from https://www.crd.york.ac.uk/PROSPERO/#recordDetails .
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




Similar articles
-
Impact of combined epidural anaesthesia/analgesia on postoperative cognitive impairment in patients receiving general anaesthesia: a meta-analysis of randomised controlled studies.Anaesth Crit Care Pain Med. 2022 Oct;41(5):101119. doi: 10.1016/j.accpm.2022.101119. Epub 2022 Jun 28. Anaesth Crit Care Pain Med. 2022. PMID: 35777653
-
The use of peripheral nerve block decrease incidence of postoperative cognitive dysfunction following orthopedic surgery: A systematic review and meta-analysis.BMC Anesthesiol. 2024 Oct 3;24(1):354. doi: 10.1186/s12871-024-02743-y. BMC Anesthesiol. 2024. PMID: 39358709 Free PMC article.
-
Intraoperative ketamine administration to prevent delirium or postoperative cognitive dysfunction: A systematic review and meta-analysis.Acta Anaesthesiol Scand. 2018 Oct;62(9):1182-1193. doi: 10.1111/aas.13168. Epub 2018 Jun 26. Acta Anaesthesiol Scand. 2018. PMID: 29947091
-
Penehyclidine Hydrochloride Premedication Is Not Associated with Increased Incidence of Post-Operative Cognitive Dysfunction or Delirium:A Systemic Review and Meta-Analysis.Chin Med Sci J. 2020 Jun 30;35(2):121-134. doi: 10.24920/003630. Chin Med Sci J. 2020. PMID: 32684232
-
Prevention of dexmedetomidine on postoperative delirium and early postoperative cognitive dysfunction in elderly patients undergoing hepatic lobectomy.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022 Feb 28;47(2):219-225. doi: 10.11817/j.issn.1672-7347.2022.210280. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35545412 Free PMC article. Clinical Trial. Chinese, English.
Cited by
-
Pathomechanisms of Non-Traumatic Acute Brain Injury in Critically Ill Patients.Medicina (Kaunas). 2020 Sep 13;56(9):469. doi: 10.3390/medicina56090469. Medicina (Kaunas). 2020. PMID: 32933176 Free PMC article. Review.
-
Effect of dexamethasone pretreatment using deep learning on the surgical effect of patients with gastrointestinal tumors.PLoS One. 2024 Jul 17;19(7):e0304359. doi: 10.1371/journal.pone.0304359. eCollection 2024. PLoS One. 2024. PMID: 39018292 Free PMC article.
-
[Special features of the perioperative course in patients with frailty syndrome].Anaesthesiologie. 2023 Sep;72(9):685-694. doi: 10.1007/s00101-023-01321-0. Epub 2023 Aug 18. Anaesthesiologie. 2023. PMID: 37594509 German.
-
Effects of glucocorticoids on postoperative delirium in patients undergoing elective non-cardiac surgery:A systematic review and meta-analysis.Heliyon. 2024 Dec 5;10(24):e40914. doi: 10.1016/j.heliyon.2024.e40914. eCollection 2024 Dec 30. Heliyon. 2024. PMID: 39735626 Free PMC article.
-
Effects of Glucocorticoids on Postoperative Neurocognitive Disorders in Adult Patients: A Systematic Review and Meta-Analysis.Front Aging Neurosci. 2022 Jun 30;14:939848. doi: 10.3389/fnagi.2022.939848. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35847684 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
