

The left atrial substrate plays a significant role in the development of complex atrial tachycardia in patients with precapillary pulmonary hypertension
- PMID: 31253083
- PMCID: PMC6599239
- DOI: 10.1186/s12872-019-1142-z
The left atrial substrate plays a significant role in the development of complex atrial tachycardia in patients with precapillary pulmonary hypertension
Abstract
Background: Atrial fibrillation (AF) and related atrial tachyarrhythmias (AT), including type I atrial flutter (AFL) are frequently observed in patients with pulmonary hypertension (PH). Their relationship to hemodynamic changes, atrial size, and ventricular function are still not fully verified.
Methods: We retrospectively studied hemodynamic data, echocardiographic findings and arrhythmia incidence in 814 patients with invasively diagnosed precapillary PH (aged 59 ± 14 years; 46% males). Patients with combined or post-capillary PH were excluded.
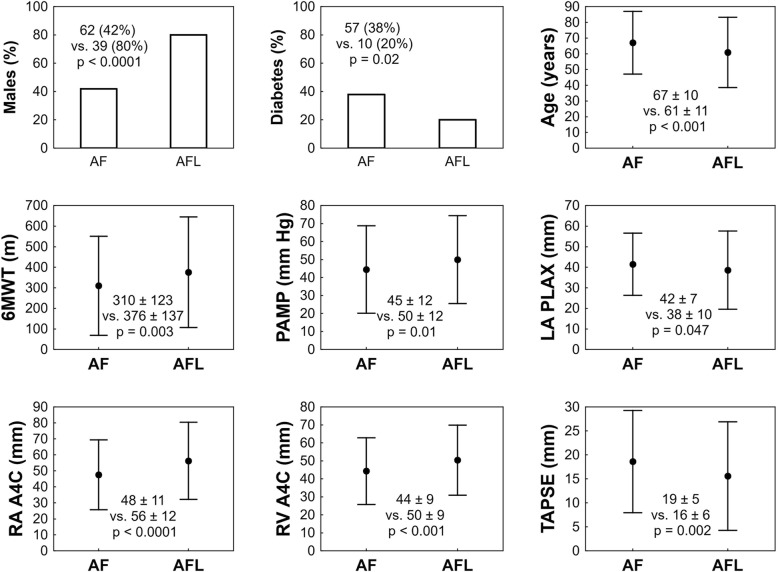
Results: AF / AT were identified in 225 (28%) of all the study population. Compared to the subgroup without arrhythmia, patients with AF / AT had elevated right atrial pressure (11 ± 5 vs. 9 ± 5 mmHg), wedge pressure (11 ± 3 vs. 10 ± 3), a more enlarged right atrium (50 ± 12 vs. 47 ± 11 mm) and an increased left atrial diameter in the parasternal long axis projection, p < 0.05 for all comparisons. In the multivariate model, the left atrial size, patient age, arterial hypertension, diabetes and type of PH were associated with AF / AT occurrence, p < 0.05. Patients with type I AFL were more frequently male (39 (80%) vs. 62 (42%)), were younger (61 ± 11 vs. 67 ± 10 years), had increased pulmonary artery mean pressure (50 ± 12 vs. 45 ± 12 mmHg), less advanced left atrial dilatation (38 ± 10 vs. 42 ± 7 mm), and a more enlarged right atrium (56 ± 12 vs. 48 ± 11) as compared to subjects with AF or other AT, p < 0.05.
Conclusions: The evidence of elevated wedge pressure and the enlargement of the left atrium especially in patients with AF suggest a parallel involvement of the left atrial substrate in arrhythmia formation despite invasively confirmed evidence of purely isolated precapillary PH. Substantial differences were noticed between patients with type I AFL and the remaining patients with other arrhythmia types.
Keywords: Atrial fibrillation; Atrial flutter; Atrial tachycardia; Pulmonary hypertension.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
The Role of Pulmonary Artery Wedge Pressure on the Incidence of Atrial Fibrillation and Atrial Tachycardias in Patients With Isolated Pre-capillary Pulmonary Hypertension.Physiol Res. 2021 Dec 30;70(6):841-849. doi: 10.33549/physiolres.934706. Epub 2021 Oct 30. Physiol Res. 2021. PMID: 34717065 Free PMC article.
-
Atrial arrhythmias in patients with arrhythmogenic right ventricular cardiomyopathy: Prevalence, echocardiographic predictors, and treatment.J Cardiovasc Electrophysiol. 2019 Oct;30(10):1801-1810. doi: 10.1111/jce.14069. Epub 2019 Jul 24. J Cardiovasc Electrophysiol. 2019. PMID: 31310380
-
Atrial arrhythmias after lung transplant: underlying mechanisms, risk factors, and prognosis.J Heart Lung Transplant. 2014 Jul;33(7):734-40. doi: 10.1016/j.healun.2014.02.032. Epub 2014 Mar 4. J Heart Lung Transplant. 2014. PMID: 24755110
-
Atrial fibrillation inducibility during cavotricuspid isthmus-dependent atrial flutter ablation as a predictor of clinical atrial fibrillation. A meta-analysis.J Interv Card Electrophysiol. 2017 Apr;48(3):307-315. doi: 10.1007/s10840-016-0211-9. Epub 2017 Jan 9. J Interv Card Electrophysiol. 2017. PMID: 28070875 Review.
-
Prevalence of atrial arrhythmia in patients with arrhythmogenic right ventricular cardiomyopathy: a systematic review and meta-analysis.J Cardiovasc Med (Hagerstown). 2020 May;21(5):368-376. doi: 10.2459/JCM.0000000000000962. J Cardiovasc Med (Hagerstown). 2020. PMID: 32243340
Cited by
-
Left atrial ablation for the management of atrial tachyarrhythmias in patients with pulmonary hypertension: A case series.HeartRhythm Case Rep. 2022 Jan 27;8(4):275-279. doi: 10.1016/j.hrcr.2022.01.012. eCollection 2022 Apr. HeartRhythm Case Rep. 2022. PMID: 35497477 Free PMC article. No abstract available.
-
The impact of atrial fibrillation and atrial tachycardias on the hemodynamic status of patients with pulmonary hypertension.Physiol Res. 2022 Dec 16;71(6):791-799. doi: 10.33549/physiolres.934941. Epub 2022 Oct 13. Physiol Res. 2022. PMID: 36281725 Free PMC article.
-
The Role of Atrial Fibrosis for Atrial Fibrillation: Not Always Essential?Arq Bras Cardiol. 2024 Jan 5;120(10):e20230766. doi: 10.36660/abc.20230766. Arq Bras Cardiol. 2024. PMID: 38198354 Free PMC article. English, Portuguese. No abstract available.
-
Atrial fibrillation and atrial tachycardia in patients with chronic thromboembolic pulmonary hypertension treated with pulmonary endarterectomy.Eur Heart J Suppl. 2020 Jul;22(Suppl F):F30-F37. doi: 10.1093/eurheartj/suaa096. Epub 2020 Jul 15. Eur Heart J Suppl. 2020. PMID: 32694951 Free PMC article.
-
The Role of Pulmonary Artery Wedge Pressure on the Incidence of Atrial Fibrillation and Atrial Tachycardias in Patients With Isolated Pre-capillary Pulmonary Hypertension.Physiol Res. 2021 Dec 30;70(6):841-849. doi: 10.33549/physiolres.934706. Epub 2021 Oct 30. Physiol Res. 2021. PMID: 34717065 Free PMC article.
References
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37(1):67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
