

Topping-off surgery vs posterior lumbar interbody fusion for degenerative lumbar disease: a comparative study of clinical efficacy and adjacent segment degeneration
- PMID: 31253158
- PMCID: PMC6599350
- DOI: 10.1186/s13018-019-1245-3
Topping-off surgery vs posterior lumbar interbody fusion for degenerative lumbar disease: a comparative study of clinical efficacy and adjacent segment degeneration
Abstract
Background: Studies have shown that adjacent segment degeneration (ASD) is a common complication after posterior lumbar interbody fusion (PLIF), even a second surgery is required for some patients. It remains unclear whether the non-fusion surgery can relieve ASD. Therefore, this study aims to investigate the clinical outcomes of Topping-off surgery (fusion combined with Coflex) and PLIF for degenerative lumbar disease (DLD) and the efficacy on preventing ASD.
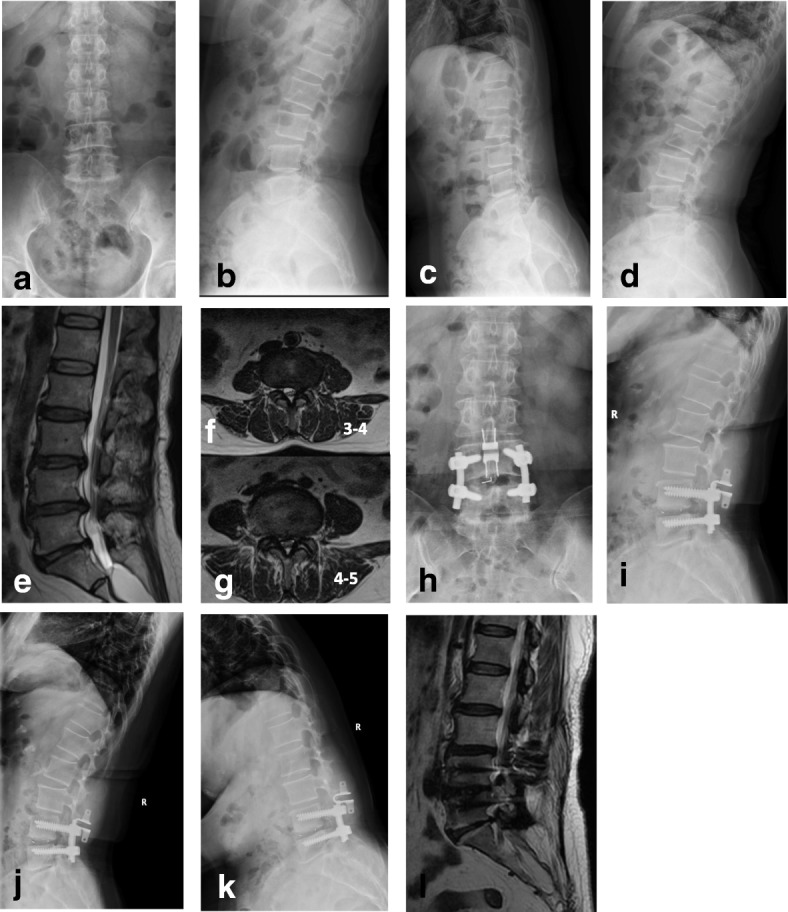
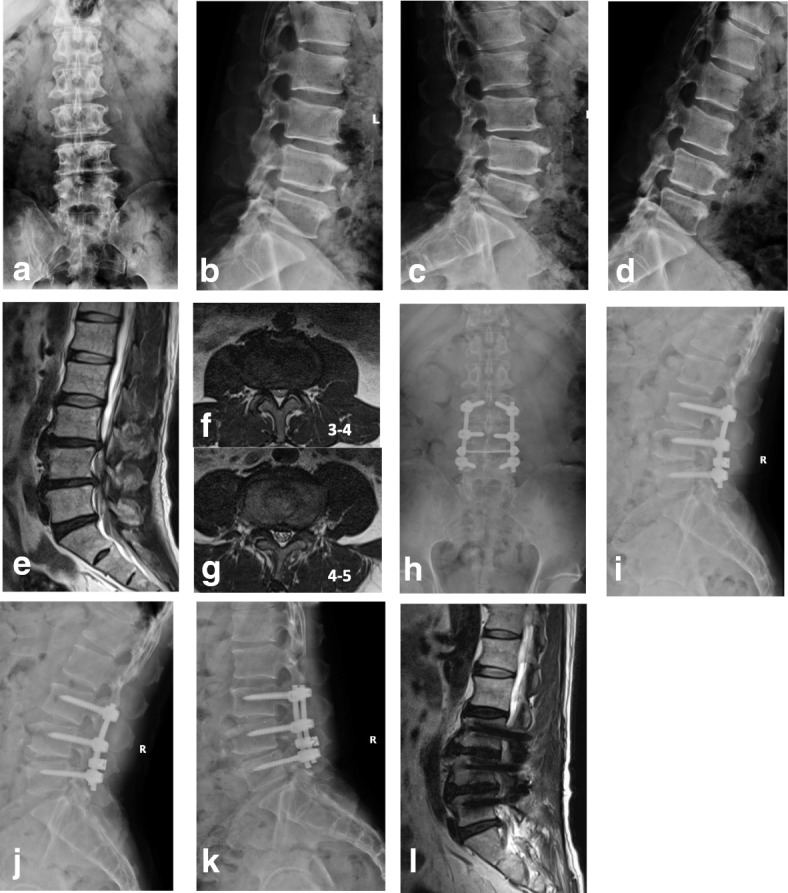
Method: A retrospective analysis was performed on the clinical data of 99 patients with DLD from January 2011 to December 2014, who were performed by Topping-off surgery (L4-5 PLIF + L3-4 Coflex, n = 45) or PLIF (L3-5 PLIF, n = 54). All patients included in the analysis had a minimum of 3 years of follow-up. Clinical data were used to assess the clinical efficacy, and radiographic parameters were measured for evaluation of the incidence of ASD.
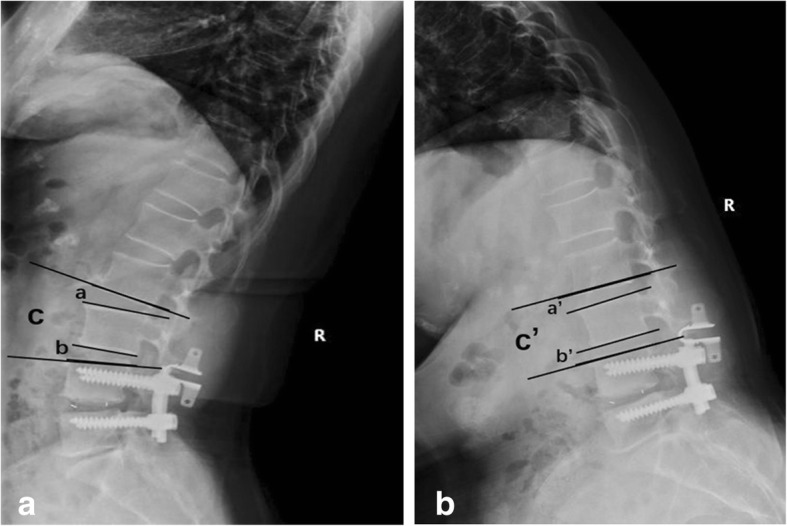
Results: The mean ages of Topping-off group and PLIF group were 53.5 and 65.7 years old, respectively (P < 0.05). The surgical time, intraoperative blood loss, Oswestry disability index (ODI), and visual analog scale (VAS) were significantly different between the two groups (P < 0.05). Intervertebral mobility (L2-L3) of the Topping-off group was not changed significantly at 3 years after surgery than before (P > 0.05), while that of PLIF group was increased considerably (P < 0.05). As to intergroup comparison, intervertebral mobility (L2-L3) of Topping-off group was superior to those of the PLIF group (P < 0.05). Surprisingly, there was no significant difference in the general adjacent segment mobility (GASM) at L2-4 of the Topping-off group and intervertebral mobility (L2-L3) of PLIF group at 3 years after surgery (P > 0.05). Lumbar MRI at three post-operative years indicated that the modified Pfirrman grading of disc (L2-L3) in the Topping-off group was much better than that of the PLIF group (P < 0.05).
Conclusion: This study showed that Topping-off surgery had the benefits of less invasiveness, less bleeding, and comparable clinical efficacy as PLIF for DLD. The segment with Coflex insertion undertook part of the mobility and stress in the proximal lumbar spine, which is conducive to alleviating ASD.
Keywords: Adjacent segment degeneration (ASD); Clinical efficacy; Coflex; Degenerative lumbar disease (DLD); Posterior lumbar interbody fusion (PLIF); Topping-off.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Topping-Off Technology versus Posterior Lumbar Interbody Fusion in the Treatment of Lumbar Disc Herniation: A Meta-Analysis.Biomed Res Int. 2020 Jan 13;2020:2953128. doi: 10.1155/2020/2953128. eCollection 2020. Biomed Res Int. 2020. PMID: 32420333 Free PMC article.
-
Topping-off surgery vs posterior lumbar interbody fusion for degenerative lumbar disease: a finite element analysis.J Orthop Surg Res. 2019 Dec 30;14(1):476. doi: 10.1186/s13018-019-1503-4. J Orthop Surg Res. 2019. PMID: 31888664 Free PMC article.
-
Reduction in adjacent-segment degeneration after multilevel posterior lumbar interbody fusion with proximal DIAM implantation.J Neurosurg Spine. 2015 Aug;23(2):190-6. doi: 10.3171/2014.12.SPINE14666. Epub 2015 May 1. J Neurosurg Spine. 2015. PMID: 25932598
-
Comparison of Topping-off and posterior lumbar interbody fusion surgery in lumbar degenerative disease: a retrospective study.Chin Med J (Engl). 2012 Nov;125(22):3942-6. Chin Med J (Engl). 2012. PMID: 23158121
-
Dynamic Stabilization Adjacent to Fusion versus Posterior Lumbar Interbody Fusion for the Treatment of Lumbar Degenerative Disease: A Meta-Analysis.Biomed Res Int. 2020 May 20;2020:9309134. doi: 10.1155/2020/9309134. eCollection 2020. Biomed Res Int. 2020. PMID: 32550234 Free PMC article.
Cited by
-
Percutaneous Endoscopic Transforaminal Lumbar Interbody Fusion: Technique Note and Comparison of Early Outcomes with Minimally Invasive Transforaminal Lumbar Interbody Fusion for Lumbar Spondylolisthesis.Int J Gen Med. 2021 Feb 22;14:549-558. doi: 10.2147/IJGM.S298591. eCollection 2021. Int J Gen Med. 2021. PMID: 33654422 Free PMC article.
-
Effectiveness of Interspinous Process Devices in Managing Adjacent Segment Degeneration Following Lumbar Spinal Fusion: A Systematic Review and Meta-Analysis.J Clin Med. 2024 Aug 30;13(17):5160. doi: 10.3390/jcm13175160. J Clin Med. 2024. PMID: 39274374 Free PMC article. Review.
-
New combination of IntraSPINE device and posterior lumbar interbody fusion for rare skipped-level lumbar disc herniation: a case report and literature review.J Int Med Res. 2020 Aug;48(8):300060520949764. doi: 10.1177/0300060520949764. J Int Med Res. 2020. PMID: 32856512 Free PMC article. Review.
-
Topping-Off Technology versus Posterior Lumbar Interbody Fusion in the Treatment of Lumbar Disc Herniation: A Meta-Analysis.Biomed Res Int. 2020 Jan 13;2020:2953128. doi: 10.1155/2020/2953128. eCollection 2020. Biomed Res Int. 2020. PMID: 32420333 Free PMC article.
-
Preoperative Nutritional Status Screened by MNA-SF Predicts Major Complications in Elderly Patients Undergoing Lumbar Fusion Surgery.Clin Interv Aging. 2024 Dec 3;19:2031-2042. doi: 10.2147/CIA.S481610. eCollection 2024. Clin Interv Aging. 2024. PMID: 39649110 Free PMC article.
References
-
- Mo Z, Li D, Zhang R, et al. Comparative effectiveness and safety of posterior lumbar interbody fusion, Coflex, Wallis, and X-stop for lumbar degenerative diseases: a systematic review and network meta-analysis. Clin Neurol Neurosurg. 2018;172:74–81. doi: 10.1016/j.clineuro.2018.06.030. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
