

Matched-Pair Comparison of 68Ga-PSMA-11 PET/CT and 18F-PSMA-1007 PET/CT: Frequency of Pitfalls and Detection Efficacy in Biochemical Recurrence After Radical Prostatectomy
- PMID: 31253741
- PMCID: PMC6954457
- DOI: 10.2967/jnumed.119.229187
Matched-Pair Comparison of 68Ga-PSMA-11 PET/CT and 18F-PSMA-1007 PET/CT: Frequency of Pitfalls and Detection Efficacy in Biochemical Recurrence After Radical Prostatectomy
Abstract
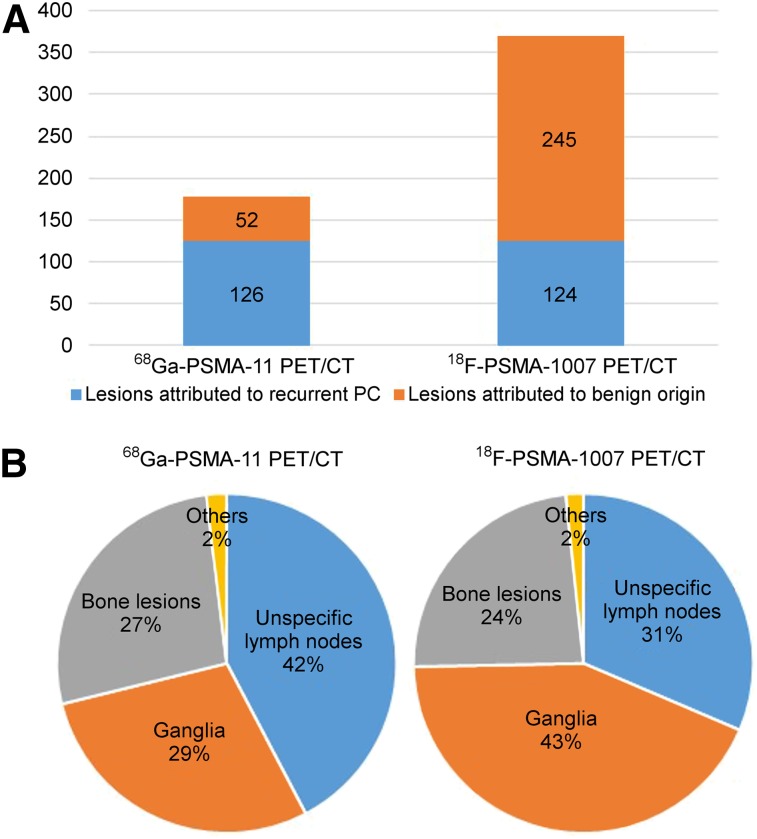
18F-labeled prostate-specific membrane antigen (PSMA)-ligand PET has several principal advantages over 68Ga-PSMA-11. The purpose of this retrospective study was to evaluate the frequency of non-tumor-related uptake and the detection efficacy comparing 68Ga-PSMA-11 PET/CT and 18F-PSMA-1007 PET/CT in recurrent prostate cancer (PC) patients. Methods: The study included 102 patients with biochemically recurrent PC after radical prostatectomy undergoing 18F-PSMA-1007 PET/CT imaging. On the basis of various clinical variables, patients with corresponding 68Ga-PSMA-11 PET/CT scans were matched. All PET/CT scans (n = 204) were reviewed by 1 nuclear medicine physician. First, all PET-positive lesions were noted. Then, lesions suspected of being recurrent PC were differentiated from lesions attributed to a benign origin on the basis of known pitfalls and information from CT. For each region, the SUVmax of the lesion with the highest PSMA-ligand uptake was noted. Detection rates were determined, and SUVmax was compared separately for 68Ga-PSMA-11 and 18F-PSMA-1007. Results: In total, 18F-PSMA-1007 PET and 68Ga-PSMA-11 PET revealed 369 and 178 PSMA-ligand-positive lesions, respectively. 18F-PSMA-1007 PET revealed approximately 5 times more lesions attributed to a benign origin than did 68Ga-PSMA-11 PET (245 vs. 52 lesions, respectively). The benign lesions most frequently observed were ganglia, unspecific lymph node, and bone lesions, at a rate of 43%, 31%, and 24% for 18F-PSMA-1007 PET and 29%, 42%, and 27% for 68Ga-PSMA-11 PET, respectively. The SUVmax of lesions attributed to a benign origin was significantly higher (P < 0.0001) for 18F-PSMA-1007 PET. Further, a similar number of lesions was attributed to recurrent PC (124/369 for 18F-PSMA-1007 PET and 126/178 for 68Ga-PSMA-11 PET). Conclusion: The number of lesions with increased PSMA-ligand uptake attributed to a benign origin is considerably higher for 18F-PSMA-1007 PET than for 68Ga-PSMA-11 PET. This finding indicates the need for sophisticated reader training emphasizing known pitfalls and reporting within the clinical context.
Keywords: PET/CT; PSMA; genitourinary; oncology; pitfalls; prostate cancer.
© 2020 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Han M, Partin AW, Zahurak M, et al. Biochemical (prostate specific antigen) recurrence probability following radical prostatectomy for clinically localized prostate cancer. J Urol. 2003;169:517–523. - PubMed
-
- Briganti A, Abdollah F, Nini A, et al. Performance characteristics of computed tomography in detecting lymph node metastases in contemporary patients with prostate cancer treated with extended pelvic lymph node dissection. Eur Urol. 2012;61:1132–1138. - PubMed
-
- Perera M, Papa N, Christidis D, et al. Sensitivity, specificity, and predictors of positive 68Ga-prostate-specific membrane antigen positron emission tomography in advanced prostate cancer: a systematic review and meta-analysis. Eur Urol. 2016;70:926–937. - PubMed
-
- Hofman MS, Hicks RJ, Maurer T, et al. Prostate-specific membrane antigen PET: clinical utility in prostate cancer, normal patterns, pearls, and pitfalls. Radiographics. 2018;38:200–217. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous