

Feasibility of a Real-Time Clinical Augmented Reality and Artificial Intelligence Framework for Pain Detection and Localization From the Brain
- PMID: 31254336
- PMCID: PMC6625219
- DOI: 10.2196/13594
Feasibility of a Real-Time Clinical Augmented Reality and Artificial Intelligence Framework for Pain Detection and Localization From the Brain
Abstract
Background: For many years, clinicians have been seeking for objective pain assessment solutions via neuroimaging techniques, focusing on the brain to detect human pain. Unfortunately, most of those techniques are not applicable in the clinical environment or lack accuracy.
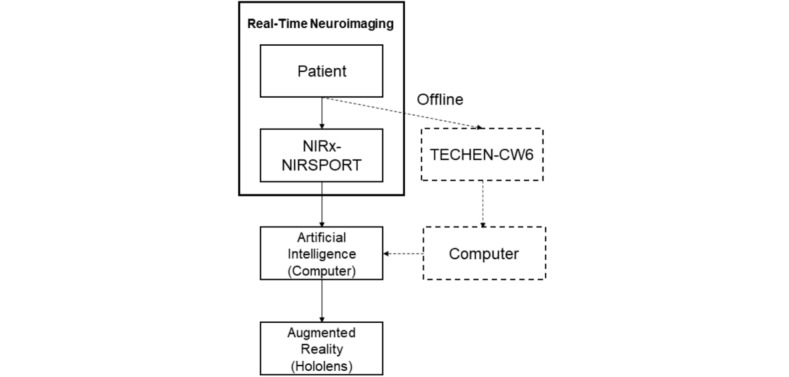
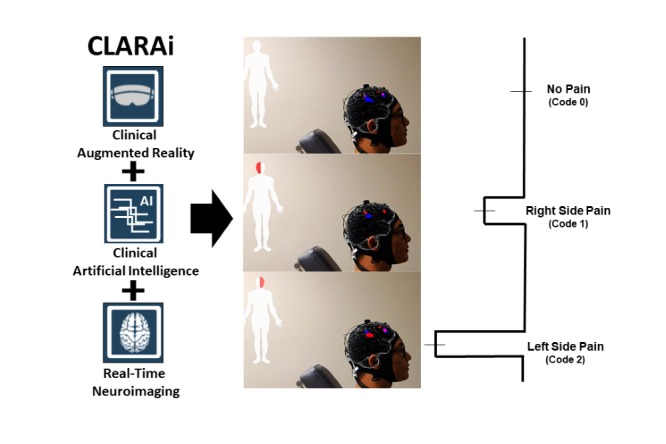
Objective: This study aimed to test the feasibility of a mobile neuroimaging-based clinical augmented reality (AR) and artificial intelligence (AI) framework, CLARAi, for objective pain detection and also localization direct from the patient's brain in real time.
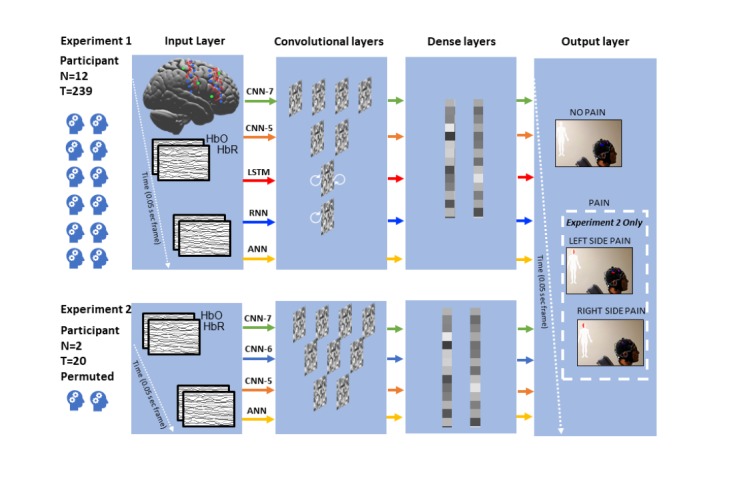
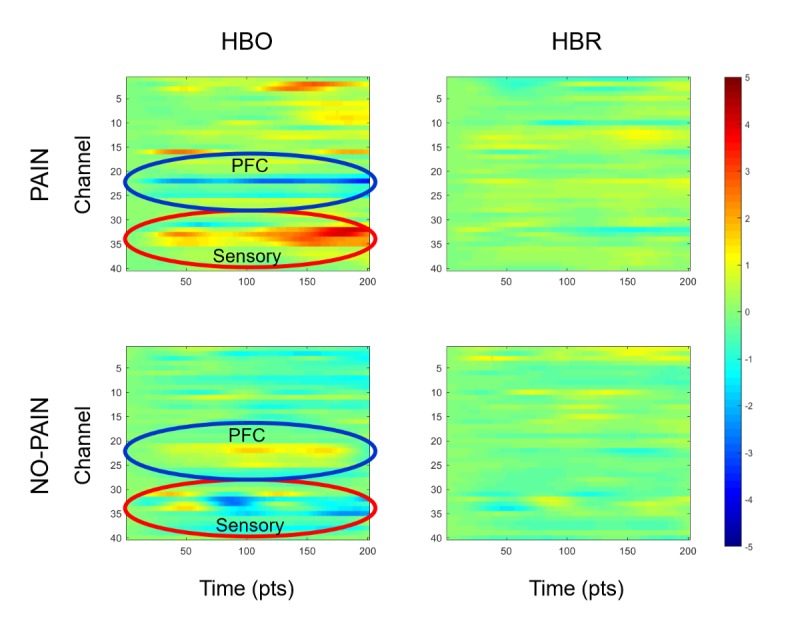
Methods: Clinical dental pain was triggered in 21 patients by hypersensitive tooth stimulation with 20 consecutive descending cold stimulations (32°C-0°C). We used a portable optical neuroimaging technology, functional near-infrared spectroscopy, to gauge their cortical activity during evoked acute clinical pain. The data were decoded using a neural network (NN)-based AI algorithm to classify hemodynamic response data into pain and no-pain brain states in real time. We tested the performance of several networks (NN with 7 layers, 6 layers, 5 layers, 3 layers, recurrent NN, and long short-term memory network) upon reorganized data features on pain diction and localization in a simulated real-time environment. In addition, we also tested the feasibility of transmitting the neuroimaging data to an AR device, HoloLens, in the same simulated environment, allowing visualization of the ongoing cortical activity on a 3-dimensional brain template virtually plotted on the patients' head during clinical consult.
Results: The artificial neutral network (3-layer NN) achieved an optimal classification accuracy at 80.37% (126,000/156,680) for pain and no pain discrimination, with positive likelihood ratio (PLR) at 2.35. We further explored a 3-class localization task of left/right side pain and no-pain states, and convolutional NN-6 (6-layer NN) achieved highest classification accuracy at 74.23% (1040/1401) with PLR at 2.02.
Conclusions: Additional studies are needed to optimize and validate our prototype CLARAi framework for other pains and neurologic disorders. However, we presented an innovative and feasible neuroimaging-based AR/AI concept that can potentially transform the human brain into an objective target to visualize and precisely measure and localize pain in real time where it is most needed: in the doctor's office.
International registered report identifier (irrid): RR1-10.2196/13594.
Keywords: artificial intelligence; pain; spectroscopy, near-infrared; virtual reality.
©Xiao-Su Hu, Thiago D Nascimento, Mary C Bender, Theodore Hall, Sean Petty, Stephanie O’Malley, Roger P Ellwood, Niko Kaciroti, Eric Maslowski, Alexandre F DaSilva. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 28.06.2019.
Conflict of interest statement
Conflicts of Interest: The content described within this study has been developed at the UM and disclosed to the UM Office of Technology Transfer. All intellectual property rights including but not limited to patents/patent applications, trademark and copyright of software, algorithms, reports, displays, and visualizations are owned by the Regents of the University of Michigan. Drs DaSilva and Maslowski are the co-creators of CLARAi. Drs DaSilva and Malowski are co-founders of MoxyTech Inc, which has optioned the technology CLARAi from University of Michigan. Dr. Roger P Ellwood, who was previously an employee of the Colgate Palmolive company-the funding agency of this work.
Figures
References
-
- Nascimento TD, DosSantos MF, Danciu T, DeBoer M, van Holsbeeck H, Lucas SR, Aiello C, Khatib L, Bender MA, UMSoD (Under)Graduate Class Of 2014. Zubieta J, DaSilva AF. Real-time sharing and expression of migraine headache suffering on Twitter: a cross-sectional infodemiology study. J Med Internet Res. 2014 Apr;16(4):e96. doi: 10.2196/jmir.3265. http://www.jmir.org/2014/4/e96/ v16i4e96 - DOI - PMC - PubMed
-
- Wager TD, Atlas LY, Lindquist MA, Roy M, Woo C, Kross E. An fMRI-based neurologic signature of physical pain. N Engl J Med. 2013 Apr 11;368(15):1388–97. doi: 10.1056/NEJMoa1204471. http://europepmc.org/abstract/MED/23574118 - DOI - PMC - PubMed
-
- Harper DE, Shah Y, Ichesco E, Gerstner GE, Peltier SJ. Multivariate classification of pain-evoked brain activity in temporomandibular disorder. Pain Rep. 2016 Sep;1(3) doi: 10.1097/PR9.0000000000000572. http://europepmc.org/abstract/MED/28630949 - DOI - PMC - PubMed
-
- Davis KD, Flor H, Greely HT, Iannetti GD, Mackey S, Ploner M, Pustilnik A, Tracey I, Treede R, Wager TD. Brain imaging tests for chronic pain: medical, legal and ethical issues and recommendations. Nat Rev Neurol. 2017 Oct;13(10):624–638. doi: 10.1038/nrneurol.2017.122.nrneurol.2017.122 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
