

Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study
- PMID: 31257127
- PMCID: PMC6727070
- DOI: 10.1016/S0140-6736(19)30721-4
Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study
Erratum in
-
Department of Error.Lancet. 2019 Aug 31;394(10200):736. doi: 10.1016/S0140-6736(19)32010-0. Lancet. 2019. PMID: 31478499 Free PMC article. No abstract available.
Abstract
Background: Pneumonia is the leading cause of death among children younger than 5 years. In this study, we estimated causes of pneumonia in young African and Asian children, using novel analytical methods applied to clinical and microbiological findings.
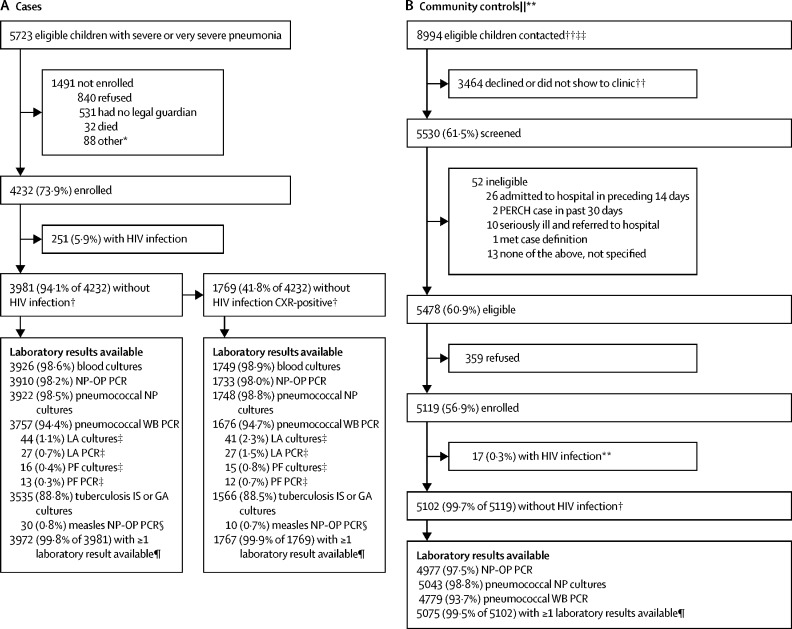
Methods: We did a multi-site, international case-control study in nine study sites in seven countries: Bangladesh, The Gambia, Kenya, Mali, South Africa, Thailand, and Zambia. All sites enrolled in the study for 24 months. Cases were children aged 1-59 months admitted to hospital with severe pneumonia. Controls were age-group-matched children randomly selected from communities surrounding study sites. Nasopharyngeal and oropharyngeal (NP-OP), urine, blood, induced sputum, lung aspirate, pleural fluid, and gastric aspirates were tested with cultures, multiplex PCR, or both. Primary analyses were restricted to cases without HIV infection and with abnormal chest x-rays and to controls without HIV infection. We applied a Bayesian, partial latent class analysis to estimate probabilities of aetiological agents at the individual and population level, incorporating case and control data.
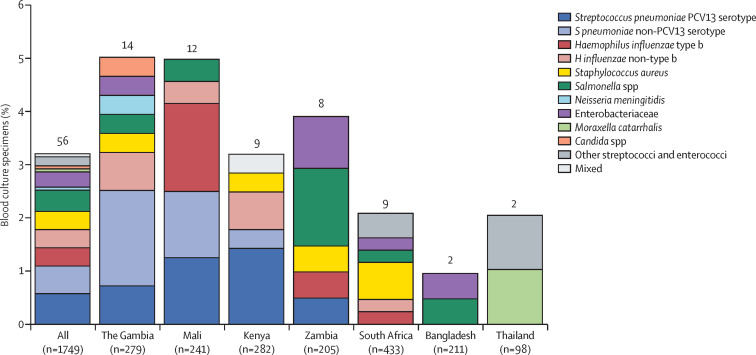
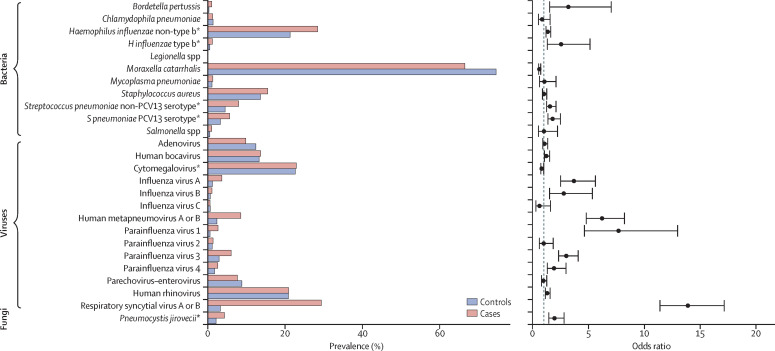
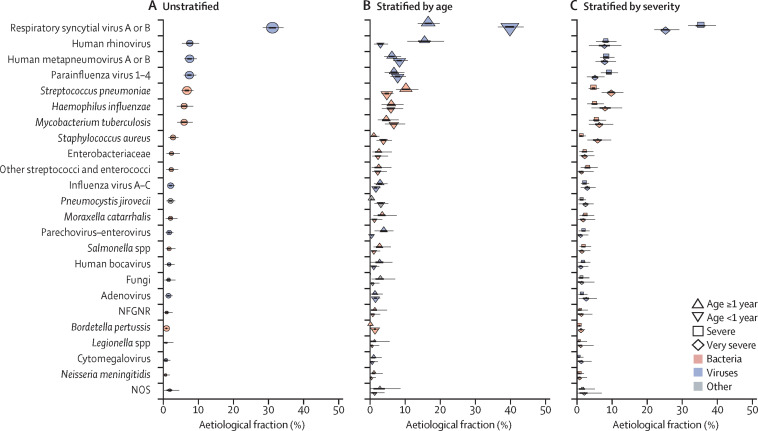
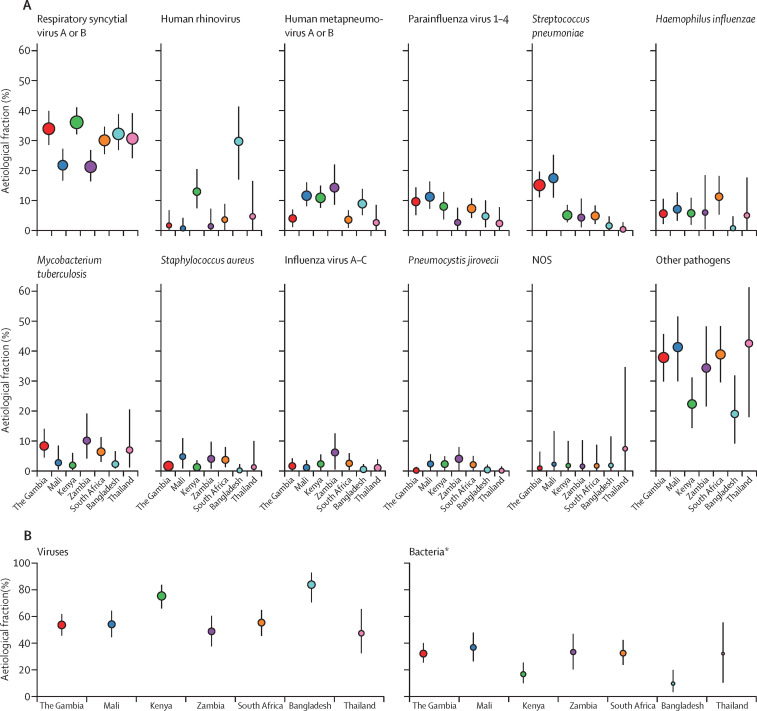
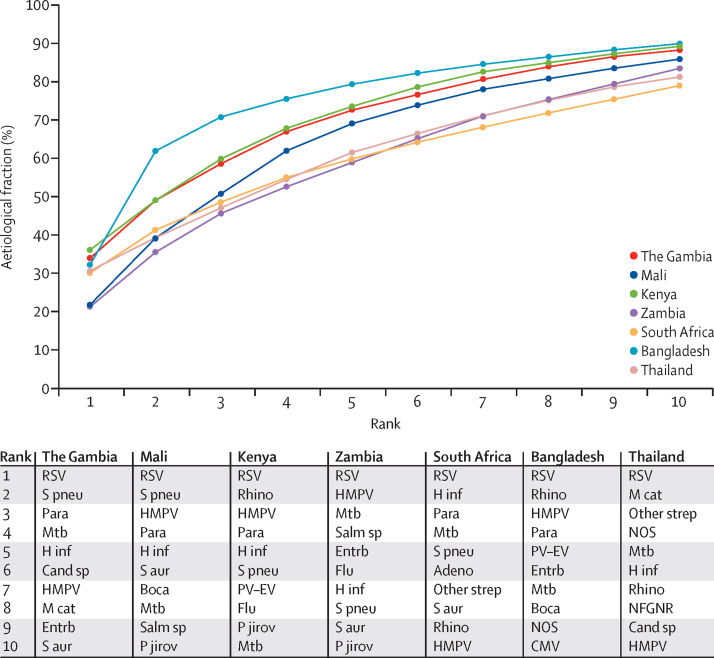
Findings: Between Aug 15, 2011, and Jan 30, 2014, we enrolled 4232 cases and 5119 community controls. The primary analysis group was comprised of 1769 (41·8% of 4232) cases without HIV infection and with positive chest x-rays and 5102 (99·7% of 5119) community controls without HIV infection. Wheezing was present in 555 (31·7%) of 1752 cases (range by site 10·6-97·3%). 30-day case-fatality ratio was 6·4% (114 of 1769 cases). Blood cultures were positive in 56 (3·2%) of 1749 cases, and Streptococcus pneumoniae was the most common bacteria isolated (19 [33·9%] of 56). Almost all cases (98·9%) and controls (98·0%) had at least one pathogen detected by PCR in the NP-OP specimen. The detection of respiratory syncytial virus (RSV), parainfluenza virus, human metapneumovirus, influenza virus, S pneumoniae, Haemophilus influenzae type b (Hib), H influenzae non-type b, and Pneumocystis jirovecii in NP-OP specimens was associated with case status. The aetiology analysis estimated that viruses accounted for 61·4% (95% credible interval [CrI] 57·3-65·6) of causes, whereas bacteria accounted for 27·3% (23·3-31·6) and Mycobacterium tuberculosis for 5·9% (3·9-8·3). Viruses were less common (54·5%, 95% CrI 47·4-61·5 vs 68·0%, 62·7-72·7) and bacteria more common (33·7%, 27·2-40·8 vs 22·8%, 18·3-27·6) in very severe pneumonia cases than in severe cases. RSV had the greatest aetiological fraction (31·1%, 95% CrI 28·4-34·2) of all pathogens. Human rhinovirus, human metapneumovirus A or B, human parainfluenza virus, S pneumoniae, M tuberculosis, and H influenzae each accounted for 5% or more of the aetiological distribution. We observed differences in aetiological fraction by age for Bordetella pertussis, parainfluenza types 1 and 3, parechovirus-enterovirus, P jirovecii, RSV, rhinovirus, Staphylococcus aureus, and S pneumoniae, and differences by severity for RSV, S aureus, S pneumoniae, and parainfluenza type 3. The leading ten pathogens of each site accounted for 79% or more of the site's aetiological fraction.
Interpretation: In our study, a small set of pathogens accounted for most cases of pneumonia requiring hospital admission. Preventing and treating a subset of pathogens could substantially affect childhood pneumonia outcomes.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
What the PERCH study means for future pneumonia strategies.Lancet. 2019 Aug 31;394(10200):714-716. doi: 10.1016/S0140-6736(19)31512-0. Epub 2019 Jun 27. Lancet. 2019. PMID: 31257128 No abstract available.
References
-
- Feikin D, Flannery B, Hamel M, Stack M, Hansen P. Disease control priorities: reproductive, maternal, newborn, and child health. 3rd. World Bank; Washington DC: 2016. Vaccines for children in low- and middle-income countries; pp. 187–204. - PubMed
-
- Lee LA, Franzel L, Atwell J. The estimated mortality impact of vaccinations forecast to be administered during 2011–2020 in 73 countries supported by the GAVI Alliance. Vaccine. 2013;31:B61–B72. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
