

Acute Hematogenous Osteomyelitis in Children
- PMID: 31258423
- PMCID: PMC6584206
- DOI: 10.31486/toj.18.0138
Acute Hematogenous Osteomyelitis in Children
Abstract
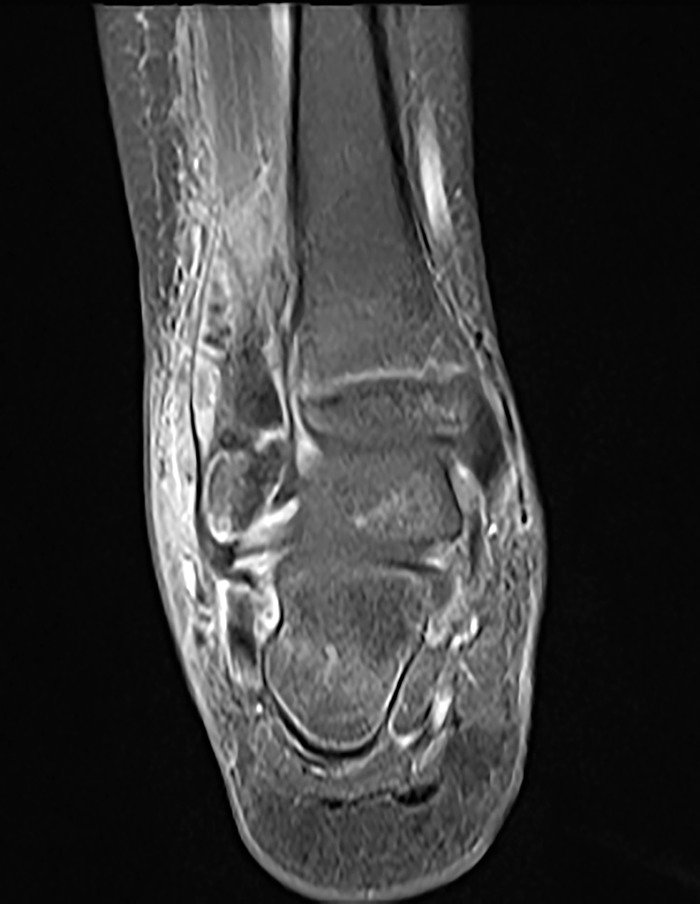
Background: The epidemiology of acute hematogenous osteomyelitis (AHO) in children has changed. Methods: We reviewed the current literature regarding the epidemiology, microbiology, pathogenesis, clinical presentation, diagnosis, and antimicrobial management of AHO in children. Results: Staphylococcus aureus is the most common microorganism causing pediatric AHO, followed by group A Streptococcus (GAS). AHO due to community-associated methicillin-resistant Staphylococcus aureus (MRSA) can cause severe and complicated disease. Pathogen isolation by culture is key for targeted antibiotic therapy. Polymerase chain reaction assay in tissue sample or joint fluid may enhance the yield of Kingella kingae. C-reactive protein is useful in diagnosis and monitoring the course of AHO. Magnetic resonance imaging is the preferred diagnostic imaging study for AHO. Clindamycin or vancomycin (for serious disease) is recommended for empiric therapy of suspected AHO due to MRSA depending on the geographic prevalence. Penicillinase-stable penicillins or first-generation cephalosporins are preferred antibiotics to treat methicillin-sensitive S aureus (MSSA) infection. Beta-lactam agents are the drugs of choice for treating AHO due to K kingae, GAS, or Streptococcus pneumoniae. For uncomplicated AHO due to MSSA, a short parenteral antibiotic course followed by oral therapy for a minimum total duration of 3-4 weeks is adequate. Complicated AHO due to MRSA may warrant prolonged therapy with surgical intervention. Conclusion: Given the evolution of pathogens, the variability in clinical presentations and course ranging from simple to complex disease, and response to treatment, the management of AHO continues to evolve and warrants an individualized, multidisciplinary approach.
Keywords: Anti-bacterial agents; methicillin-resistant staphylococcus aureus; osteomyelitis.
Figures
References
-
- Krogstad P. Osteomyelitis. In: Cherry J, Demmler-Harrison GJ, Kaplan SL, Steinbach WJ, Hotez PJ, eds. Feigin and Cherry's Textbook of Pediatric Infectious Diseases. 7th ed Philadelphia, PA: Elsevier Saunders; 2014:711-727.
-
- Hong DK, Gutierrez K. Osteomyelitis In: Long SS, Prober CG, Fischer M, eds. Principles and Practice of Pediatric Infectious Diseases. 5th ed Philadelphia, PA: Elsevier; 2018:480-486.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials