

Abnormalities of the Optic Nerve in Down Syndrome and Associations With Visual Acuity
- PMID: 31258511
- PMCID: PMC6587677
- DOI: 10.3389/fneur.2019.00633
Abnormalities of the Optic Nerve in Down Syndrome and Associations With Visual Acuity
Abstract
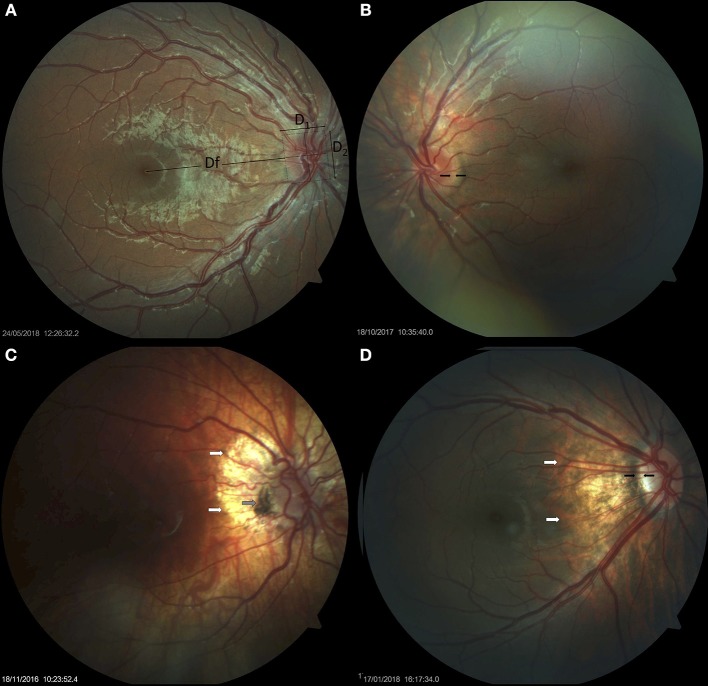
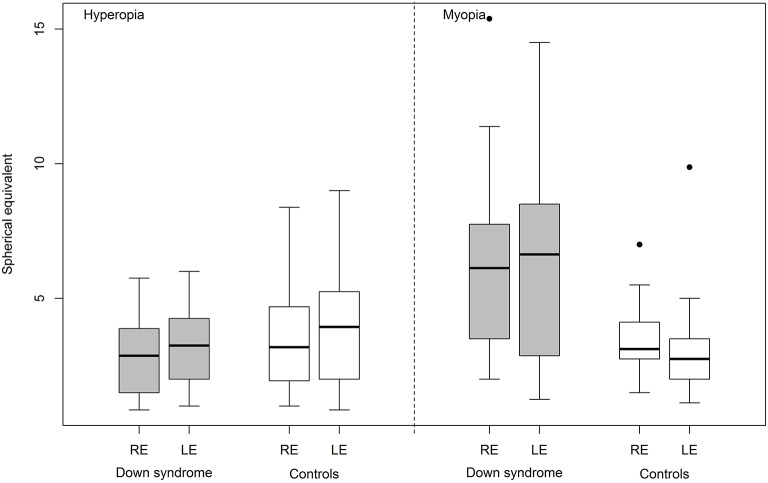
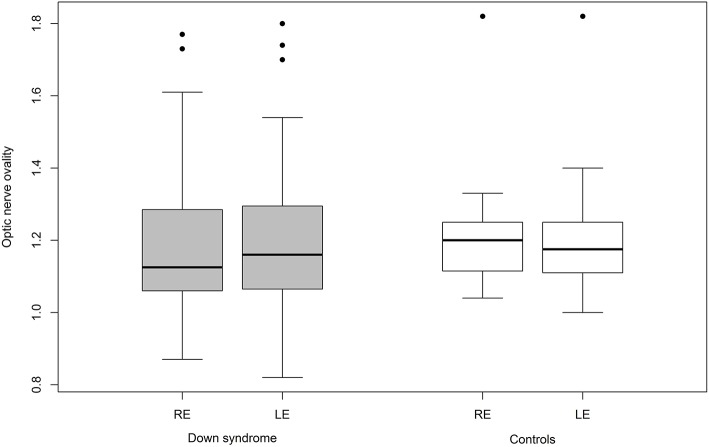
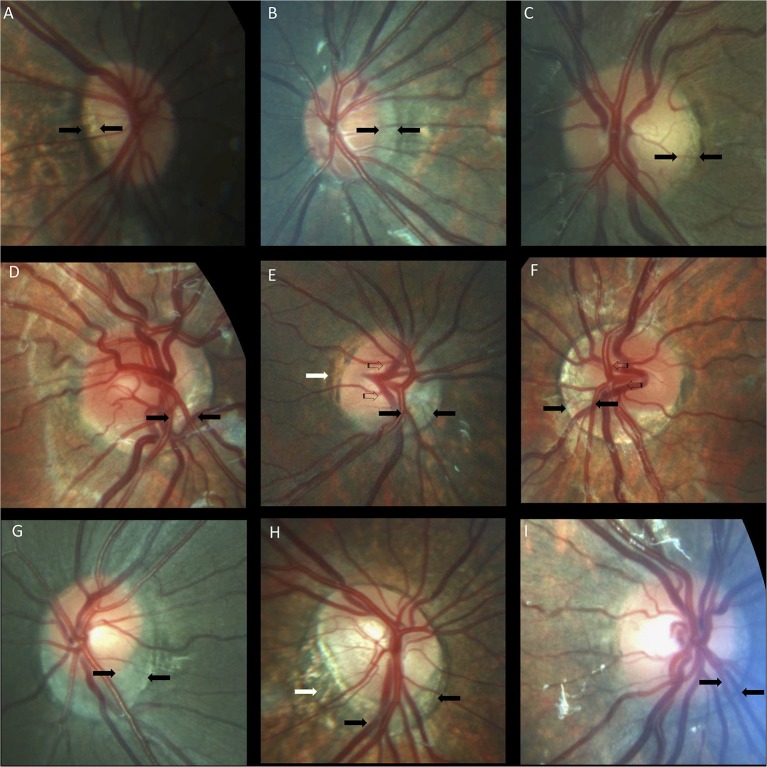
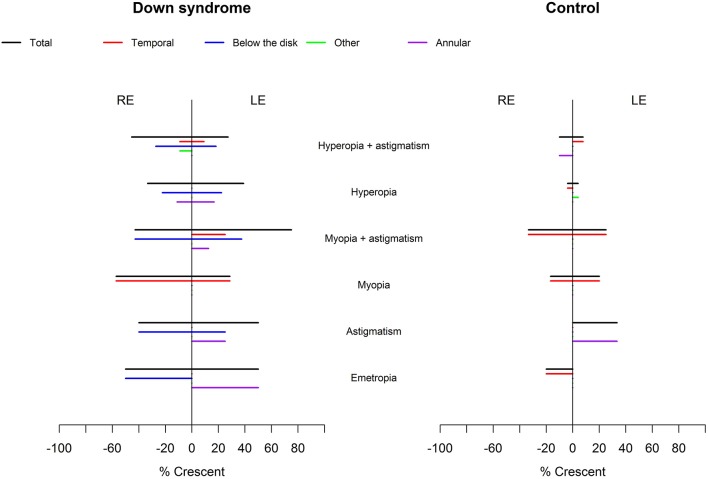
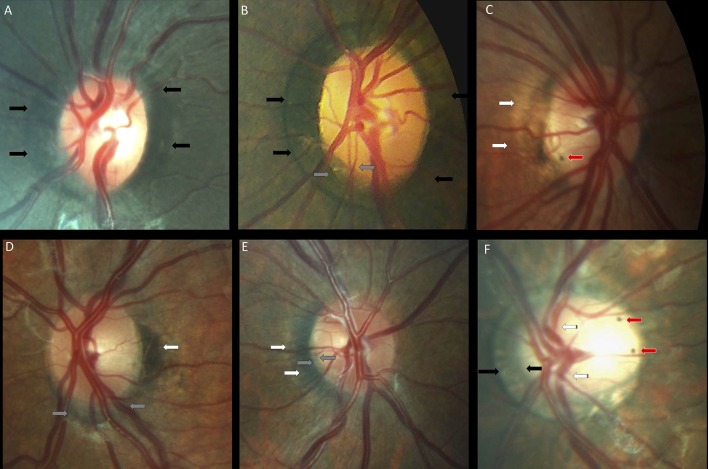
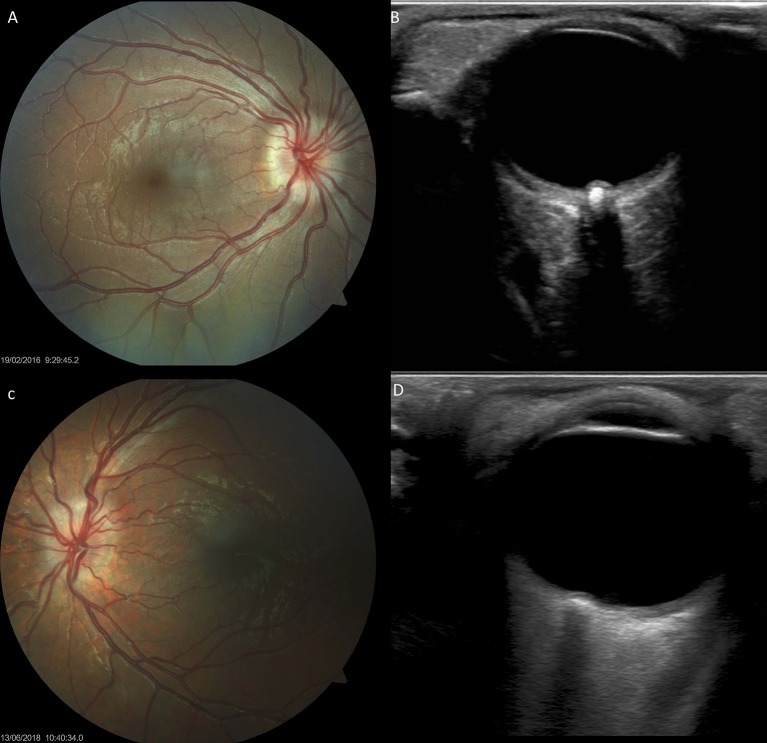
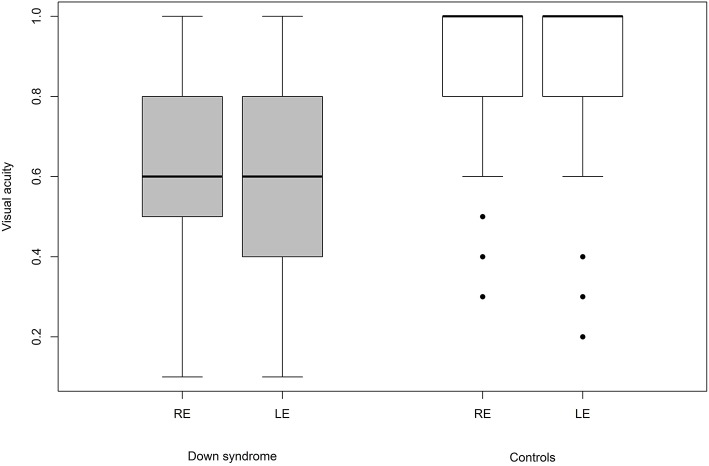
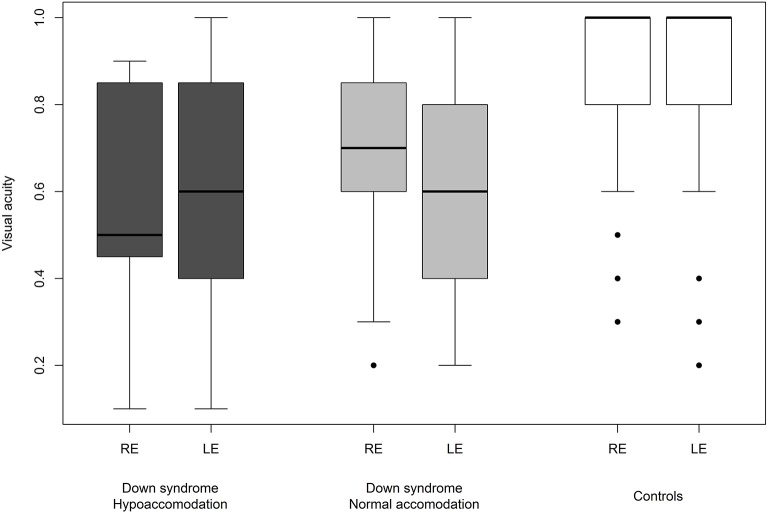
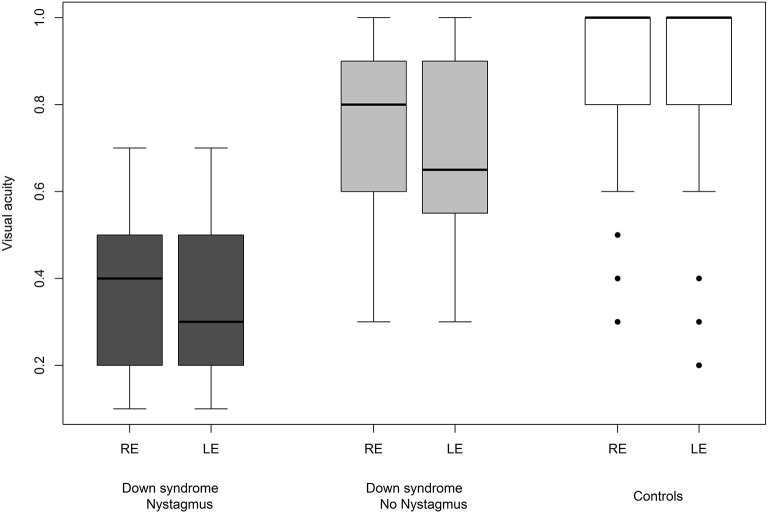
Background: Various ocular anomalies are present in the vast majority of individuals with Down syndrome; however, we know little about optic nerve abnormalities. The aim of this cross-sectional comparative study was to describe optic disc morphology in patients with Down syndrome and to determine if the differences found are potentially related to visual acuity. Subjects/methods: Assessable fundus images were obtained in 50 children with Down syndrome and 52 children without Down syndrome. Morphological analysis of the optic nerve was performed, including the disc-to-macula distance (DM) to disc diameter (DD) ratio (DM/DD), the cup-to-disc ratio and optic disc ovality. Data relating to ophthalmological status were retrospectively analyzed to evaluate the possible causes of reduced visual acuity. Results: DM/DD was significantly larger (p = 0.0036) and the cup-to-disc ratio was significantly smaller (p = 0.018) in children with Down syndrome, compared to controls. The optic discs were also more frequently torted (p = 0.034), tilted (p = 0.0049) and oval (p = 0.026). Furthermore, crescents (p = 0.0002), peripapillary atrophy (p = 0.0009), and pigment anomalies (p < 0.0001) were also more prevalent in children with Down syndrome than in those without. Visual acuity was significantly lower in children with Down syndrome compared to controls with similar refraction problems and strabismus prevalence (p < 0.0001). The mean DM/DD and the presence of a crescent was not directly related to visual acuity (r = 0.39, p = 0.31), (r = 0.35, p = 0.12) respectively. Visual acuity was diminished in 80% of children with Down syndrome and the smallest discs and in 84% of those with tilted discs. However, other causes may contribute to the diminished visual acuity in these cases. Conclusion: The optic nerve head in children with Down syndrome is affected by various anatomical and developmental abnormalities. Unrelated to refraction (spherical equivalent), the optic discs appear smaller and more frequently mal-inserted in Down syndrome. Optic disc hypoplasia, as well as severe tilting, may reduce vision but they do not represent major contributors to the decrease of vision in such children. As these children often have multiple ocular and neurosensory problems, it remains challenging to relate visual acuity problems with a specific abnormality. Smaller discs may lead to optic disc drusen formation in children with Down syndrome.
Keywords: Down syndrome; optic disc drusen; optic disc size; optic nerve; physiological cup; tilted disc; visual acuity.
Figures
Similar articles
-
Heidelberg retinal tomography of optic disc and nerve fiber layer in singapore children: variations with disc tilt and refractive error.Invest Ophthalmol Vis Sci. 2007 Nov;48(11):4939-44. doi: 10.1167/iovs.07-0585. Invest Ophthalmol Vis Sci. 2007. PMID: 17962442
-
Ocular manifestations in fetal alcohol syndrome.Eur J Ophthalmol. 2007 Jan-Feb;17(1):104-9. doi: 10.1177/112067210701700114. Eur J Ophthalmol. 2007. PMID: 17294389
-
The disc-macula distance to disc diameter ratio: a new test for confirming optic nerve hypoplasia in young children.J Pediatr Ophthalmol Strabismus. 1988 May-Jun;25(3):151-4. doi: 10.3928/0191-3913-19880501-11. J Pediatr Ophthalmol Strabismus. 1988. PMID: 3397860
-
Neuro-Ophthalmological Manifestations in Children with Down Syndrome: Current Perspectives.Eye Brain. 2021 Jul 21;13:193-203. doi: 10.2147/EB.S319817. eCollection 2021. Eye Brain. 2021. PMID: 34321946 Free PMC article. Review.
-
Optic nerve hypoplasia.Oman J Ophthalmol. 2013 May;6(2):77-82. doi: 10.4103/0974-620X.116622. Oman J Ophthalmol. 2013. PMID: 24082663 Free PMC article. Review.
Cited by
-
Prevalence and etiology of strabismus in Down syndrome: A systematic review and meta-analysis with a focus on ethnic differences in the esotropia/exotropia ratio.medRxiv [Preprint]. 2025 Apr 23:2024.11.28.24318156. doi: 10.1101/2024.11.28.24318156. medRxiv. 2025. Update in: Ophthalmic Epidemiol. 2025 Jun 3:1-19. doi: 10.1080/09286586.2025.2500018. PMID: 39649585 Free PMC article. Updated. Preprint.
-
RUN(X) out of blood: emerging RUNX1 functions beyond hematopoiesis and links to Down syndrome.Hum Genomics. 2023 Sep 5;17(1):83. doi: 10.1186/s40246-023-00531-2. Hum Genomics. 2023. PMID: 37670378 Free PMC article. Review.
-
Prevalence and Etiology of Strabismus in Down Syndrome: A Systematic Review and Meta-Analysis with a Focus on Ethnic Differences in the Esotropia/Exotropia Ratio.Ophthalmic Epidemiol. 2025 Jun 3:1-19. doi: 10.1080/09286586.2025.2500018. Online ahead of print. Ophthalmic Epidemiol. 2025. PMID: 40458862 Review.
-
Single-cell RNA sequencing of neural stem cells derived from human trisomic iPSCs reveals the abnormalities during neural differentiation of Down syndrome.Front Mol Neurosci. 2023 Jun 15;16:1137123. doi: 10.3389/fnmol.2023.1137123. eCollection 2023. Front Mol Neurosci. 2023. PMID: 37396785 Free PMC article.
-
The Ophthalmic Manifestations of Down Syndrome.Children (Basel). 2023 Feb 9;10(2):341. doi: 10.3390/children10020341. Children (Basel). 2023. PMID: 36832470 Free PMC article. Review.
References
-
- Donaldason DD. The significance of spotting of the iris in Mongolids. Brushfield's spots. Arch Ophthalmol. (1961) 65:23–31. 10.1001/archopht.1961.01840020028007 - DOI
-
- Liza-Sharmini AT, Azlan ZN, Zilfalil BA. Ocular findings in Malaysian children with Down syndrome. Singapore Med J. (2006) 47:14–9. Available online at: https://www.sma.org.sg/smj/4701/4701a1.pdf - PubMed
LinkOut - more resources
Full Text Sources
Research Materials