

The Value of Serum Immunoglobulin G Glycome in the Preoperative Discrimination of Peritoneal Metastasis from Advanced Gastric Cancer
- PMID: 31258789
- PMCID: PMC6584920
- DOI: 10.7150/jca.31380
The Value of Serum Immunoglobulin G Glycome in the Preoperative Discrimination of Peritoneal Metastasis from Advanced Gastric Cancer
Abstract
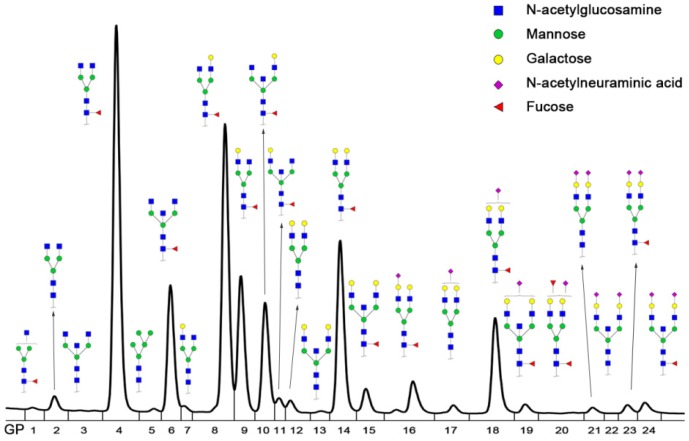
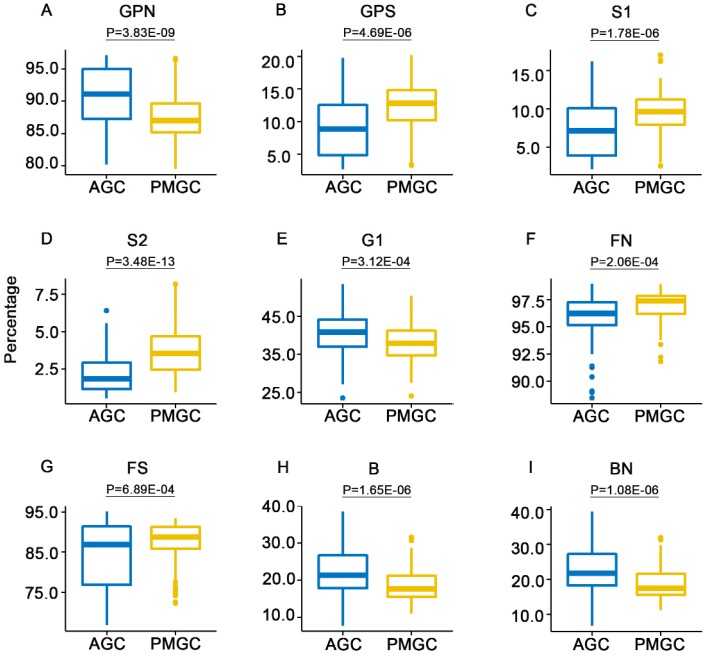
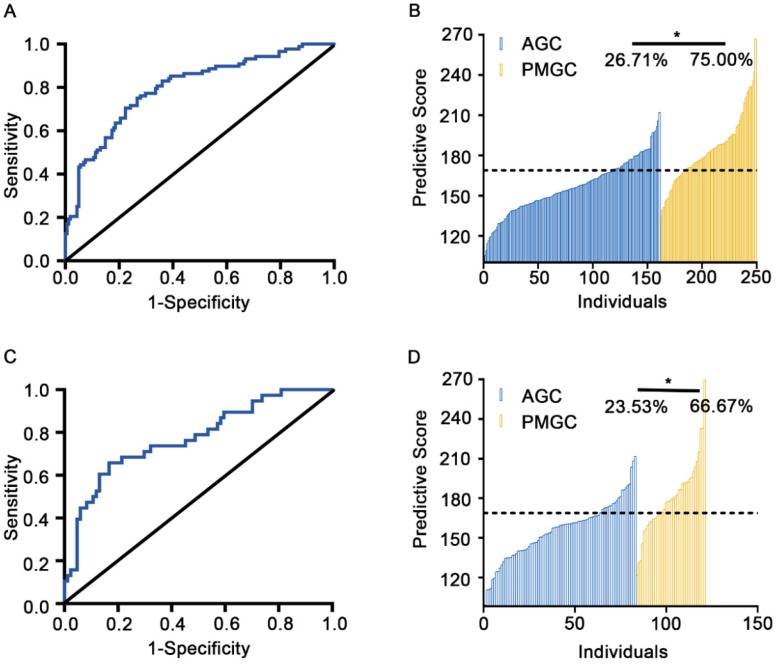
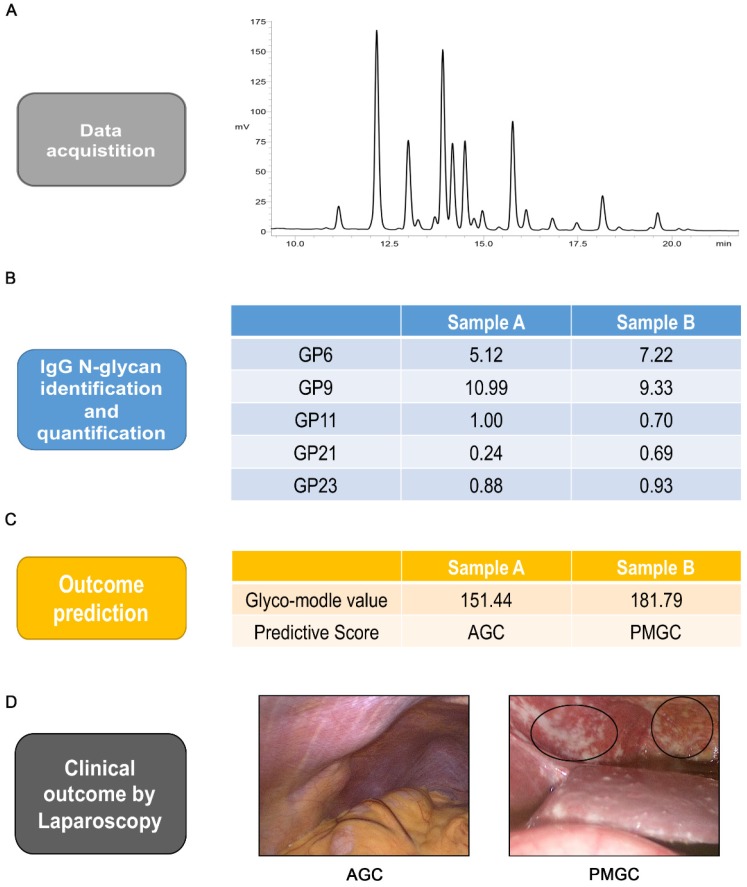
Background: Peritoneal metastasis, associated with poor prognosis in gastric cancer, is difficult to discriminate from advanced gastric cancer preoperatively. However, operative diagnosis could bring both mental and physical trauma and economic burden for patients. Consequently, a non-invasive biomarker is necessary to reduce the burden of operative diagnosis and improve survival quality of patients. This study aims to elucidate the correlation between Immunoglobulin G (IgG) N-glycome and peritoneal metastasis and find potential biomarkers in preoperative discrimination of peritoneal metastasis from advanced gastric cancer based on the comprehensive sample set. Methods: A total of 373 gastric cancer patients were enrolled and randomly sorted into training cohort (n=249) and validation cohort (n=124). The IgG N-glycome composition was analyzed by ultra-performance liquid chromatography. Results: Twenty-four glycan peaks were directly detected and 15 traits based on the same structures were evaluated between peritoneal metastasis group and advanced gastric cancer group. Several differences in IgG glycosylation were found: sialylation and fucosylation were increased in peritoneal metastasis, while neutral glycosylation, monogalacosylation and bisecting GlcNAc were decreased. Based on the significant glycomics profile, a glyco-model composed of five glycan peaks (GP6, GP9, GP11, GP21 and GP23) was established with area under the receiver operating characteristic curve (AUC) value of 0.80 (training cohort) and 0.77 (validation cohort), which showed good potential in discriminating peritoneal metastasis from advanced gastric cancer. The diagnostic performance of this model was further validated in a combined cohort (AUC=0.79). Two patients with gastric cancer were selected to perform and demonstrate the usage of the diagnostic workflow. Conclusions: Here we firstly present IgG glycome profiles in a large number of preoperative peritoneal metastasis serums. The IgG glycan was highly associated with peritoneal metastasis. These findings enhance the understanding of peritoneal metastasis. Besides, our results suggested that the newly established glyco-model could be a reliable predictor of the presence of peritoneal metastasis in patients with advanced gastric cancer.
Keywords: Biomarkers; Gastric cancer; Glycosylation; Immunoglobulin G; Peritoneal metastasis.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M. et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–86. - PubMed
-
- Maehara Y, Hasuda S, Koga T, Tokunaga E, Kakeji Y, Sugimachi K. Postoperative outcome and sites of recurrence in patients following curative resection of gastric cancer. Br J Surg. 2000;87:353–7. - PubMed
-
- Glockzin G, Piso P. Current status and future directions in gastric cancer with peritoneal dissemination. Surg Oncol Clin N Am. 2012;21:625–33. - PubMed
LinkOut - more resources
Full Text Sources
