

The burden of prostate cancer is associated with human development index: evidence from 87 countries, 1990-2016
- PMID: 31258819
- PMCID: PMC6562055
- DOI: 10.1007/s13167-019-00169-y
The burden of prostate cancer is associated with human development index: evidence from 87 countries, 1990-2016
Abstract
Aim: To examine the temporal patterns of the prostate cancer burden and its association with human development.
Subject and methods: The estimates of the incidence and mortality of prostate cancer for 87 countries were obtained from the Global Burden of Disease 2016 study for the period 1990 to 2016. The human development level of a country was measured using its human development index (HDI): a summary indicator of health, education, and income. The association between the burden of prostate cancer and the human development index (HDI) was measured using pairwise correlation and bivariate regression. Mortality-to-incidence ratio (MIR) was employed as a proxy for the survival rate of prostate cancer.
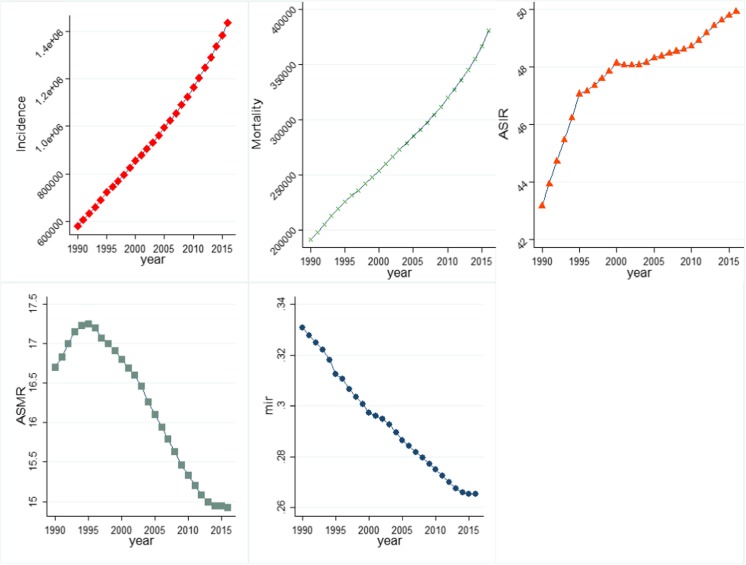
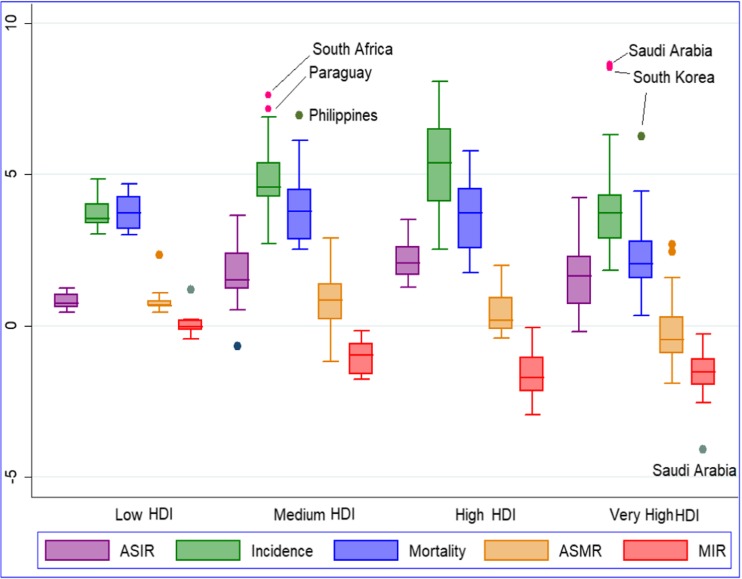
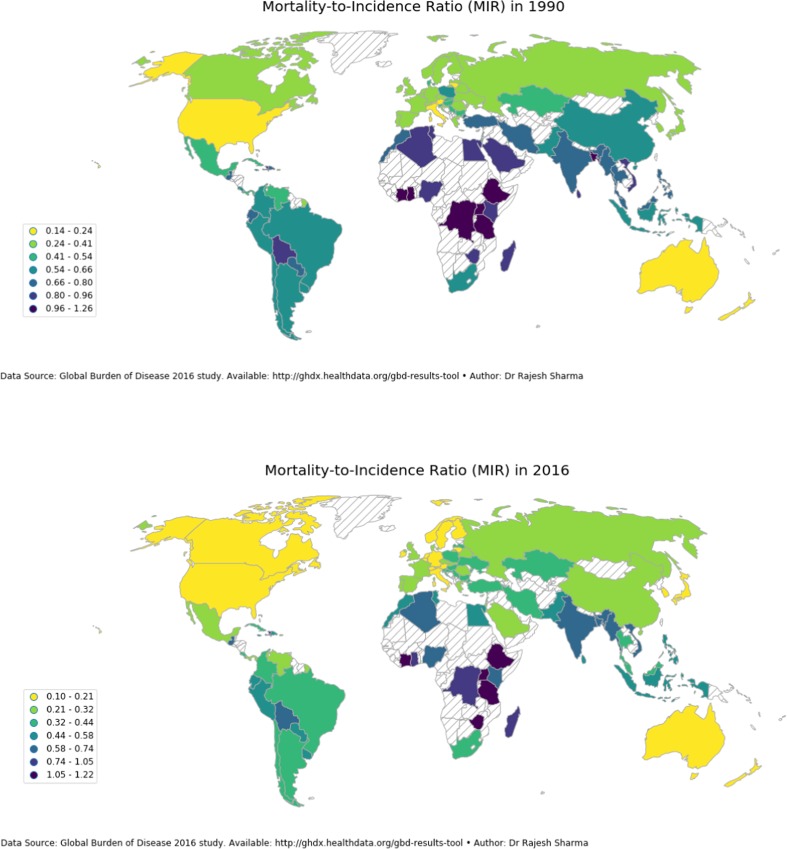
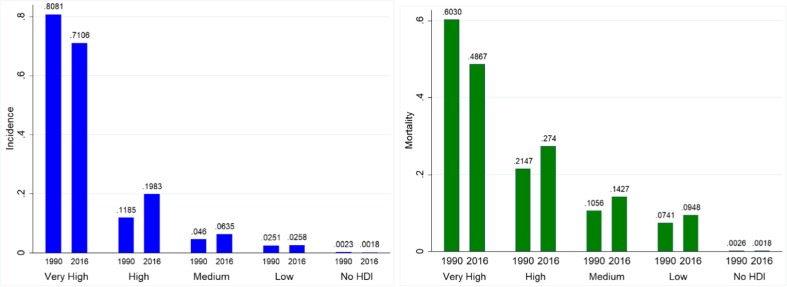
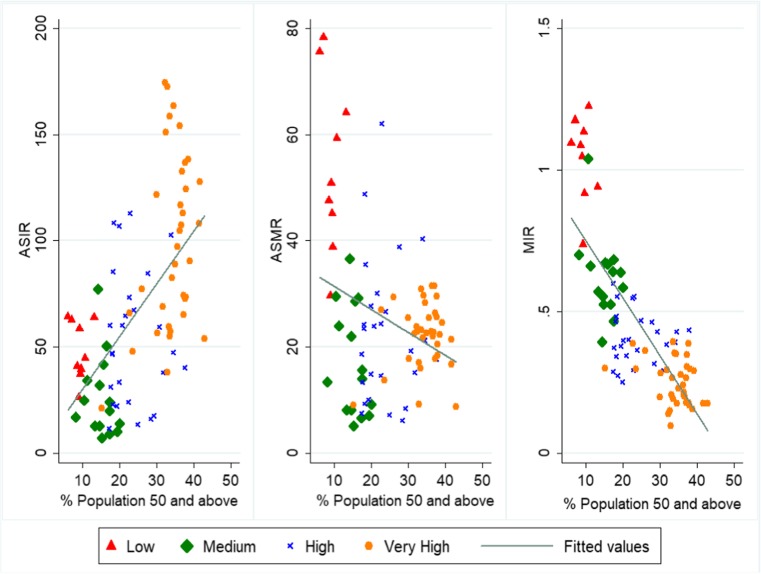
Results: Globally, 1.4 million new cases of prostate cancer arose in 2016 claiming 380,916 lives which more than doubled from 579,457 incident cases and 191,687 deaths in 1990. In 2016, the age-standardised incidence rate (ASIR) was the highest in very high-HDI countries led by Australia with ASIR of 174.1/100,000 and showed a strong positive association with HDI (r = 0.66); the age-standardised mortality rate (ASMR), however, was higher in low-HDI countries led by Zimbabwe with ASMR of 78.2/100,000 in 2016. Global MIR decreased from 0.33 in 1990 to 0.26 in 2016. Mortality-to-incidence ratio (MIR) exhibited a negative gradient (r = - 0.91) with human development index with tenfold variation globally with seven countries recording MIR in excess of 1 with the USA recording the minimum MIR of 0.10.
Conclusion: The high mortality and lower survival rates in less-developed countries demand all-inclusive solutions ranging from cost-effective early screening and detection to cost-effective cancer treatment. In tackling the rising burden of prostate cancer predictive, preventive and personalised medicine (PPPM) can play a useful role through prevention strategies, predicting PCa more precisely and accurately using a multiomic approach and risk-stratifying patients to provide personalised medicine.
Keywords: Human development index; Incidence; Mortality; Mortality-to-incidence ratio; Precision medicine; Predictive preventive personalised medicine; Prostate cancer.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflict of interest.
Figures
References
-
- Global Burden of Disease Cancer Collaborators Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016 a systematic analysis for the Global Burden of Disease Study. JAMA Oncol. 2018;4:1553. doi: 10.1001/jamaoncol.2018.2706. - DOI - PMC - PubMed
-
- Winter A, Sirri E, Jansen L, Wawroschek F, Kieschke J, Castro FA, Krilaviciute A, Holleczek B, Emrich K, Waldmann A, Brenner H. Comparison of prostate cancer survival in Germany and the USA: can differences be attributed to differences in stage distributions? BJU Int. 2017;119:550–559. doi: 10.1111/bju.13537. - DOI - PubMed
-
- Mohler JL, Bahnson RR, Boston B, Busby JE, D'Amico A, Eastham JA, Enke CA, George D, Horwitz EM, Huben RP, Kantoff P, Kawachi M, Kuettel M, Lange PH, MacVicar G, Plimack ER, Pow-Sang JM, Roach M, Rohren E, Roth BJ, Shrieve DC, Smith MR, Srinivas S, Twardowski P. Prostate cancer: clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2010;8:162–200. doi: 10.6004/jnccn.2010.0012. - DOI - PubMed
LinkOut - more resources
Full Text Sources
