

Availability of secondary prevention services after stroke in Europe: An ESO/SAFE survey of national scientific societies and stroke experts
- PMID: 31259259
- PMCID: PMC6572590
- DOI: 10.1177/2396987318816136
Availability of secondary prevention services after stroke in Europe: An ESO/SAFE survey of national scientific societies and stroke experts
Abstract
Background: Recurrent stroke is associated with increased disability and cognitive impairment, but the availability of secondary prevention measures after transient ischaemic attack (TIA) or stroke in Europe is uncertain. This limits prioritisation of investment and development of national stroke strategies.
Methods: National stroke representatives throughout Europe were surveyed. Consensus panels reported national data if available, or else expert opinion, estimating the availability of each intervention by quintiles of patients, dichotomised for analysis at 60%. Countries were classified into tertiles of gross domestic product per capita.
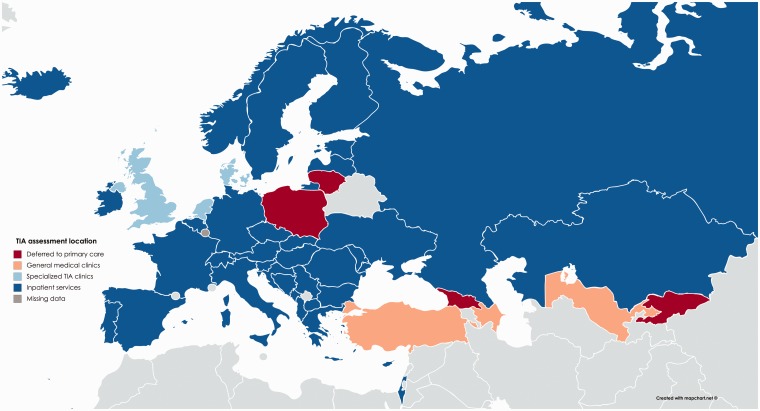
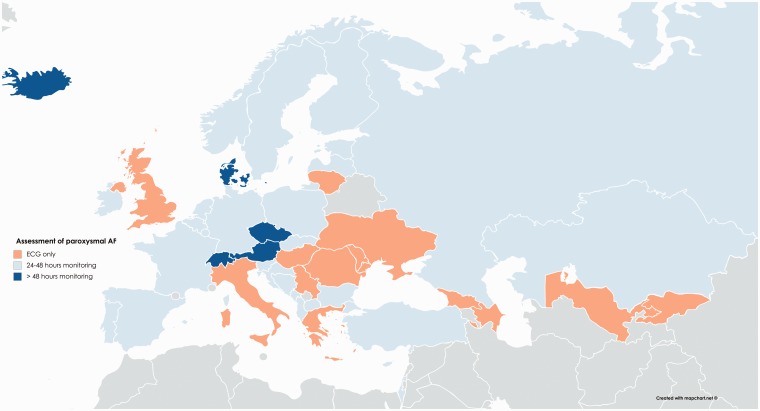
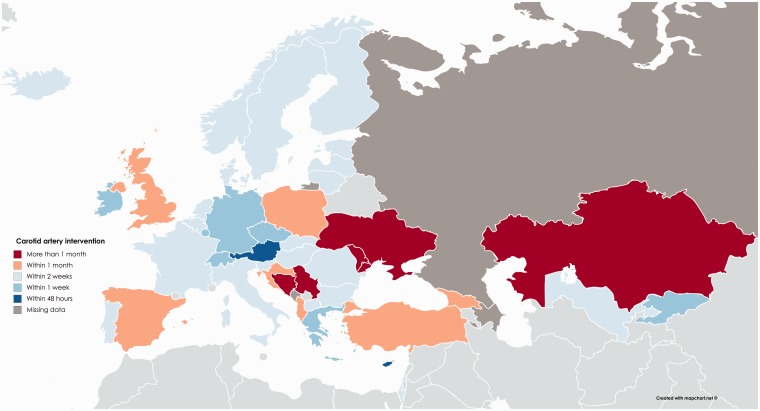
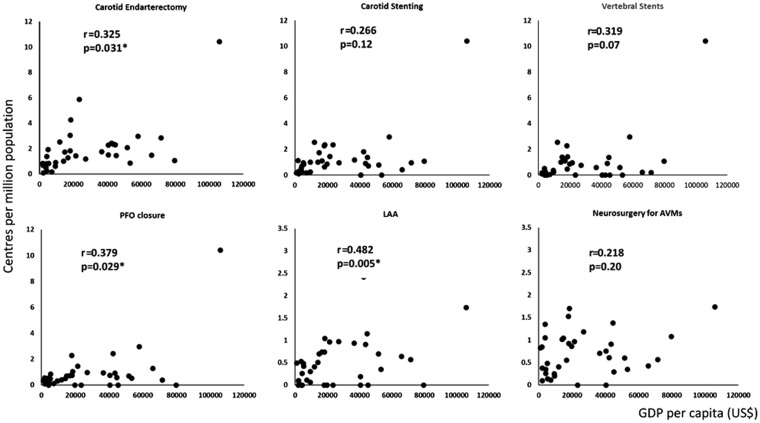
Results: Of 50 countries, 46 responded; 14/45 (31%) had national stroke registries and 25/46 (54.3%) had national stroke strategies incorporating secondary prevention. Respondents reported that the majority of TIA patients were assessed by specialist services within 48 hours in 74.4% of countries, but in nine countries more than 20% of patients were seen after more than seven days and usually assessed by non-specialists (7/46 countries). Eighty percent of countries deferred blood pressure assessment to primary care, whilst lifestyle management programmes were commonly available in only 46% of countries. Although basic interventions were widely available, interventions frequently not available to more than 60% of patients included: ambulatory cardiac monitoring (40% countries); prescription (26%) and continuation (46%) of statins; blood pressure control at follow-up (44%); carotid endarterectomy within one month (15%); face-to-face follow-up in hospital (33%); direct oral anticoagulants (21%). Gross domestic product per capita and reimbursement of interventions were the commonest predictors of availability of interventions.
Conclusions: Provision of secondary prevention varied, with gaps in care prevalent throughout Europe, particularly in lower income countries.
Keywords: Europe; Survey; secondary prevention; stroke.
Figures
References
-
- Stevens EEE, Wang Y, Mckevitt C, et al. ; on behalf of the Stroke Alliance for Europe. The burden of stroke in Europe. 2017. http://strokeeurope.eu/
-
- Amarenco P, Lavallee PC, Monteiro Tavares L, et al. Five-year risk of stroke after TIA or minor ischemic stroke. N Engl J Med 2018; 378: 2182–2190. - PubMed
-
- Ng YS, Tan KH, Chen C, et al. How do recurrent and first-ever strokes differ in rehabilitation outcomes? Am J Phys Med Rehabil 2016; 95: 709–717. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
