

Implementing a quality improvement initiative for the management of chronic obstructive pulmonary disease in rural Nepal
- PMID: 31259269
- PMCID: PMC6567951
- DOI: 10.1136/bmjoq-2018-000408
Implementing a quality improvement initiative for the management of chronic obstructive pulmonary disease in rural Nepal
Abstract
Background: Chronic obstructive pulmonary disease accounts for a significant portion of the world's morbidity and mortality, and disproportionately affects low/middle-income countries. Chronic obstructive pulmonary disease management in low-resource settings is suboptimal with diagnostics, medications and high-quality, evidence-based care largely unavailable or unaffordable for most people. In early 2016, we aimed to improve the quality of chronic obstructive pulmonary disease management at Bayalpata Hospital in rural Achham, Nepal. Given that quality improvement infrastructure is limited in our setting, we also aimed to model the use of an electronic health record system for quality improvement, and to build local quality improvement capacity.
Design: Using international chronic obstructive pulmonary disease guidelines, the quality improvement team designed a locally adapted chronic obstructive pulmonary disease protocol which was subsequently converted into an electronic health record template. Over several Plan-Do-Study-Act cycles, the team rolled out a multifaceted intervention including educational sessions, reminders, as well as audits and feedback.
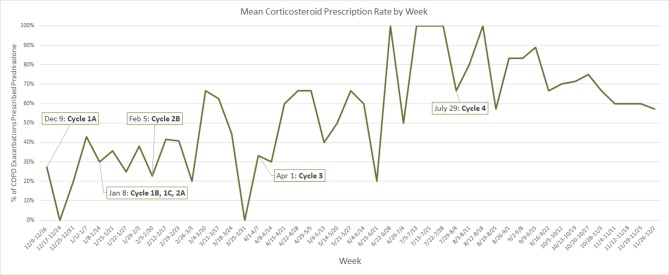
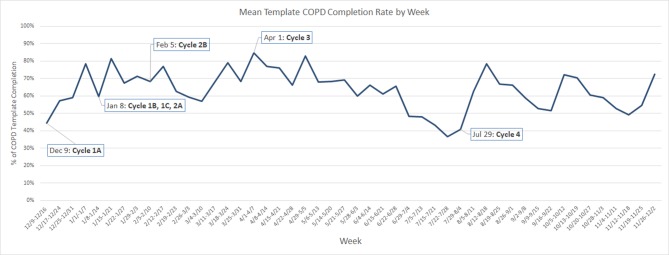
Results: The rate of oral corticosteroid prescriptions for acute exacerbations of chronic obstructive pulmonary disease increased from 14% at baseline to >60% by month 7, with the mean monthly rate maintained above this level for the remainder of the initiative. The process measure of chronic obstructive pulmonary disease template completion rate increased from 44% at baseline to >60% by month 2 and remained between 50% and 70% for the remainder of the initiative.
Conclusion: This case study demonstrates the feasibility of robust quality improvement programmes in rural settings and the essential role of capacity building in ensuring sustainability. It also highlights how individual quality improvement initiatives can catalyse systems-level improvements, which in turn create a stronger foundation for continuous quality improvement and healthcare system strengthening.
Keywords: PDSA; chronic disease management; continuous quality improvement; decision support, computerised; evidence-based medicine.
Conflict of interest statement
Competing interests: SM, AK, GD, RS, LW, DM and DS work in partnership with and DJ, NC, BD, SKD, BG, TKG, SH, SK, RM, SP, AR and AT are employed by a non-profit healthcare company (Possible) that delivers free healthcare in rural Nepal using funds from the Government of Nepal and other public, philanthropic and private foundation sources. At the time of initiative implementation, RT was employed by Possible. SM, GD, BG and LW are academic fellows affiliated to a bidirectional fellowship programme (Health, Equity, Action, Leadership Initiative Fellows) that is affiliated with a public medical school (University of California San Francisco). DJ and DRS are employed by the Government of Nepal. AK is an academic fellow at and DM is a faculty member at a private medical school (Icahn School of Medicine at Mount Sinai). GD is employed part time at a public medical centre (Natividad Medical Center). SH is employed part time at a public university (University of Washington). SK is a graduate student at a private university (Eastern University). RS and DS are faculty members at an academic medical centre (Brigham and Women’s Hospital) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. RS and DS are faculty members at a private university (Harvard Medical School). RS is employed at an academic medical centre (Massachusetts General Hospital) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. LW is employed by a medical centre (Tuba City Regional Health Care) that is managed using public sector funding through the Indian Health Services. DM is a non-voting member on Possible’s board of directors but receives no compensation. DS is employed at an academic medical centre (Beth Israel Deaconess Medical Center) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. DS is employed at an academic research centre (Ariadne Labs) that is jointly supported by an academic medical centre (Brigham and Women’s Hospital) and a private university (Harvard TH Chan School of Public Health) via public sector research funding and private philanthropy. All authors have read and understood BMJ Open Quality’s policy on competing interests and declare that we have no competing financial interests. The authors do, however, believe strongly that healthcare is a public good, not a private commodity.
Figures
Similar articles
-
Order Set to Improve the Care of Patients Hospitalized for an Exacerbation of Chronic Obstructive Pulmonary Disease.Ann Am Thorac Soc. 2016 Jun;13(6):811-5. doi: 10.1513/AnnalsATS.201507-466OC. Ann Am Thorac Soc. 2016. PMID: 27058777
-
Retrospective audit of antimicrobial prescribing practices for acute exacerbations of chronic obstructive pulmonary diseases in a large regional hospital.J Clin Pharm Ther. 2017 Jun;42(3):301-305. doi: 10.1111/jcpt.12514. Epub 2017 Mar 1. J Clin Pharm Ther. 2017. PMID: 28251670
-
Diagnosis and management of chronic obstructive pulmonary disease (COPD) in a primary care clinic.COPD. 2009 Dec;6(6):446-51. doi: 10.3109/15412550903341455. COPD. 2009. PMID: 19938968
-
Corticosteroid therapy and chronic obstructive pulmonary disease.Respir Care. 2006 Mar;51(3):289-96. Respir Care. 2006. PMID: 16533419 Review.
-
Promoting physiologic-physical adaptation in chronic obstructive pulmonary disease: pharmacotherapeutic evidence-based research and guidelines.Home Healthc Nurse. 2005 Aug;23(8):523-31; quiz 532-3. doi: 10.1097/00004045-200508000-00013. Home Healthc Nurse. 2005. PMID: 16103803 Review.
Cited by
-
Using Theories, Models, and Frameworks to Inform Implementation Cycles of Computerized Clinical Decision Support Systems in Tertiary Health Care Settings: Scoping Review.J Med Internet Res. 2023 Oct 18;25:e45163. doi: 10.2196/45163. J Med Internet Res. 2023. PMID: 37851492 Free PMC article.
-
Implementing lung health interventions in low- and middle-income countries: a FRESH AIR systematic review and meta-synthesis.Eur Respir J. 2020 Jul 23;56(1):2000127. doi: 10.1183/13993003.00127-2020. Print 2020 Jul. Eur Respir J. 2020. PMID: 32341109 Free PMC article.
-
Towards precision in defining COPD exacerbations.Breathe (Sheff). 2021 Sep;17(3):210081. doi: 10.1183/20734735.0081-2021. Breathe (Sheff). 2021. PMID: 35035551 Free PMC article. Review.
References
-
- Vos T, Allen C, Arora M, et al. . Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1545–602. 10.1016/S0140-6736(16)31678-6 - DOI - PMC - PubMed
-
- Soriano JB, Abajobir AA, Abate KH, et al. . Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med 2017;5:691–706. 10.1016/S2213-2600(17)30293-X - DOI - PMC - PubMed
-
- World Health Organization, Nepal. WHO statistical profile. http://www.who.int/gho/countries/npl.pdf
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical