

Progressive Cortical Thinning in Patients With Focal Epilepsy
- PMID: 31260004
- PMCID: PMC6604082
- DOI: 10.1001/jamaneurol.2019.1708
Progressive Cortical Thinning in Patients With Focal Epilepsy
Abstract
Importance: It is controversial whether epilepsy is a static or progressive disease. Evidence of progressive gray matter loss in epilepsy would support early diagnosis, rapid treatment, and early referral for surgical interventions.
Objective: To demonstrate progressive cortical thinning in patients with focal epilepsy distinct from cortical thinning associated with normal aging.
Design, setting, and participants: A case-control neuroimaging study was conducted from August 3, 2004, to January 26, 2016, among 190 patients with focal epilepsy at a tertiary epilepsy referral center (epilepsy data) and 3 independent comparison cohorts matched for age and sex (healthy volunteer data; n = 141).
Exposures: Two or more high-resolution T1-weighted magnetic resonance imaging scans at least 6 months apart (mean [SD] interval, 2.5 [1.6] years).
Main outcomes and measures: Global and vertexwise rate of progressive cortical thinning.
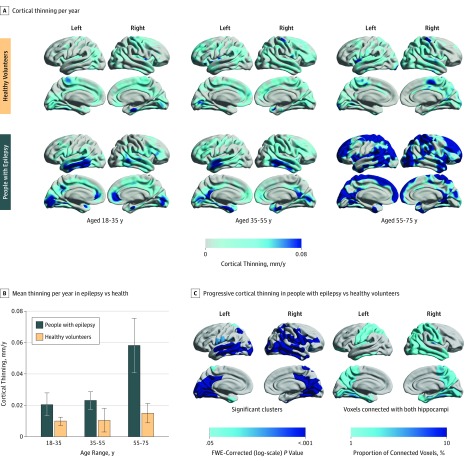
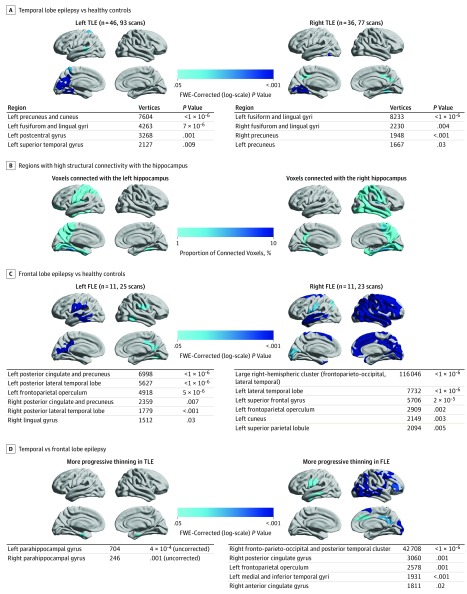
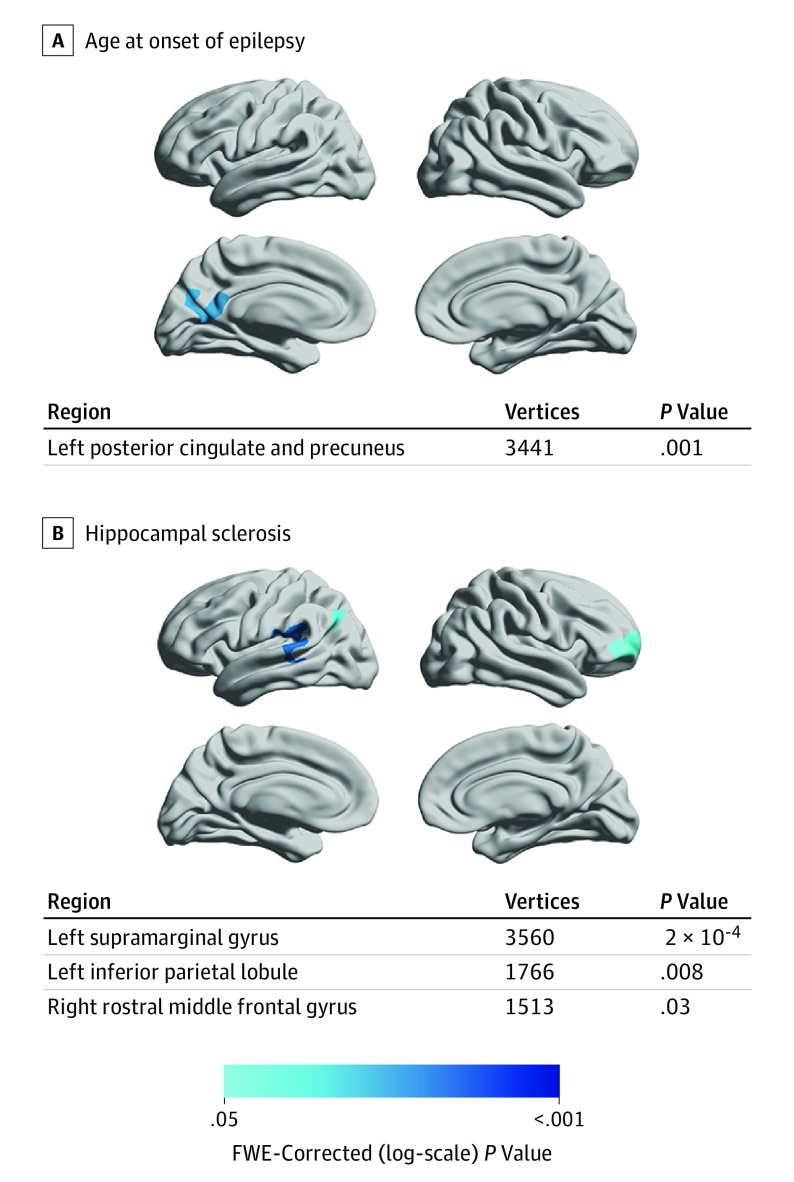
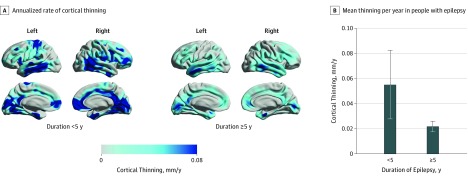
Results: A total of 190 people with focal epilepsy (99 women and 91 men; mean [SD] age, 36 [11] years; 396 magnetic resonance imaging scans) were compared with 141 healthy volunteers (76 women and 65 men; mean [SD] age, 35 [17] years; 282 magnetic resonance imaging scans). Widespread highly significant progressive cortical thinning exceeding normal aging effects, mainly involving the bilateral temporal lobes, medial parietal and occipital cortices, pericentral gyri, and opercula, was seen in 146 individuals with epilepsy (76.8%; 95% CI, 58%-95%). The mean (SD) annualized rate of global cortical thinning in patients with epilepsy was twice the rate of age-associated thinning observed in healthy volunteers (0.024 [0.061] vs 0.011 [0.029] mm/y; P = .01). Progression was most pronounced in adults older than 55 years and during the first 5 years after the onset of seizures. Areas of accelerated cortical thinning were detected in patients with early onset of epilepsy and in patients with hippocampal sclerosis. Accelerated thinning was not associated with seizure frequency, history of generalized seizures, or antiepileptic drug load and did not differ between patients with or without ongoing seizures. Progressive atrophy in temporal (n = 101) and frontal (n = 28) lobe epilepsy was most pronounced ipsilaterally to the epileptic focus but also affected a widespread area extending beyond the focus and commonly affected the contralateral hemisphere. For patients with temporal lobe epilepsy, accelerated cortical thinning was observed within areas structurally connected with the ipsilateral hippocampus.
Conclusions and relevance: Widespread progressive cortical thinning exceeding that seen with normal aging may occur in patients with focal epilepsy. These findings appear to highlight the need to develop epilepsy disease-modifying treatments to disrupt or slow ongoing atrophy. Longitudinal cortical thickness measurements may have the potential to serve as biomarkers for such studies.
Conflict of interest statement
Figures
References
-
- Gowers WR. Epilepsy and Other Chronic Convulsive Disorders. London, UK: J. & A. Churchill; 1881.
