

Association of Radioactive Iodine Treatment With Cancer Mortality in Patients With Hyperthyroidism
- PMID: 31260066
- PMCID: PMC6604114
- DOI: 10.1001/jamainternmed.2019.0981
Association of Radioactive Iodine Treatment With Cancer Mortality in Patients With Hyperthyroidism
Erratum in
-
Error in Abstract.JAMA Intern Med. 2019 Aug 1;179(8):1152. doi: 10.1001/jamainternmed.2019.3705. JAMA Intern Med. 2019. PMID: 31380945 Free PMC article. No abstract available.
Abstract
Importance: Radioactive iodine (RAI) has been used extensively to treat hyperthyroidism since the 1940s. Although widely considered a safe and effective therapy, RAI has been associated with elevated risks of total and site-specific cancer death among patients with hyperthyroidism.
Objective: To determine whether greater organ- or tissue-absorbed doses from RAI treatment are associated with overall and site-specific cancer mortality in patients with hyperthyroidism.
Design, setting, and participants: This cohort study is a 24-year extension of the multicenter Cooperative Thyrotoxicosis Therapy Follow-up Study, which has followed up US and UK patients diagnosed and treated for hyperthyroidism for nearly 7 decades, beginning in 1946. Patients were traced using records from the National Death Index, Social Security Administration, and other resources. After exclusions, 18 805 patients who were treated with RAI and had no history of cancer at the time of the first treatment were eligible for the current analysis. Excess relative risks (ERRs) per 100-mGy dose to the organ or tissue were calculated using multivariable-adjusted linear dose-response models and were converted to relative risks (RR = 1 + ERR). The current analyses were conducted from April 28, 2017, to January 30, 2019.
Exposures: Mean total administered activity of sodium iodide I 131 was 375 MBq for patients with Graves disease and 653 MBq for patients with toxic nodular goiter. Mean organ or tissue dose estimates ranged from 20 to 99 mGy (colon or rectum, ovary, uterus, prostate, bladder, and brain/central nervous system), to 100 to 400 mGy (pancreas, kidney, liver, stomach, female breast, lung, oral mucosa, and marrow), to 1.6 Gy (esophagus), and to 130 Gy (thyroid gland).
Main outcomes and measures: Site-specific and all solid-cancer mortality.
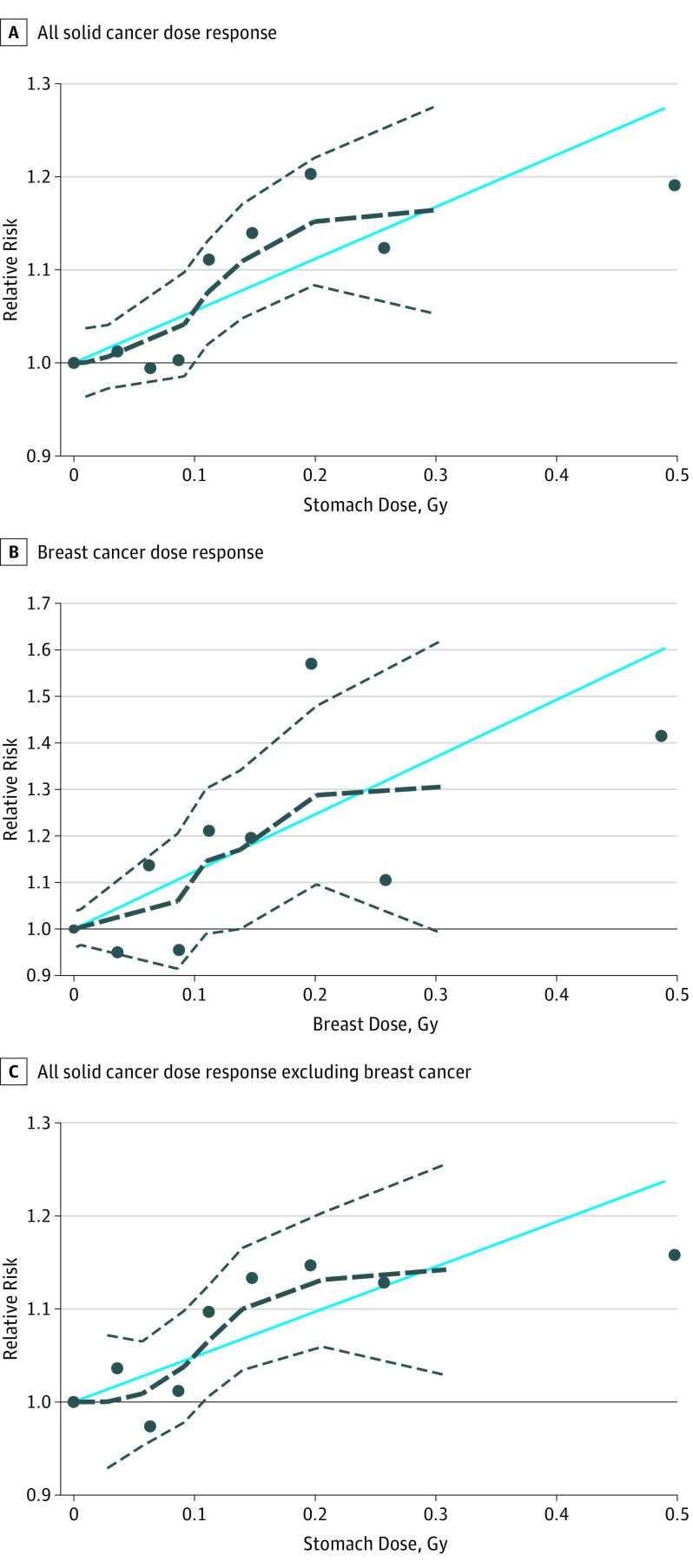
Results: A total of 18 805 patients were included in the study cohort, and the mean (SD) entry age was 49 (14) years. Most patients were women (14 671 [78.0%]), and most had a Graves disease diagnosis (17 615 [93.7%]). Statistically significant positive associations were observed for all solid cancer mortality (n = 1984; RR at 100-mGy dose to the stomach = 1.06; 95% CI, 1.02-1.10; P = .002), including female breast cancer (n = 291; RR at 100-mGy dose to the breast = 1.12; 95% CI, 1.003-1.32; P = .04) and all other solid cancers combined (n = 1693; RR at 100-mGy dose to the stomach = 1.05; 95% CI, 1.01-1.10; P = .01). The 100-mGy dose to the stomach and breast corresponded to a mean (SD) administered activity of 243 (35) MBq and 266 (58) MBq in patients with Graves disease. For every 1000 patients with hyperthyroidism receiving typical doses to the stomach (150 to 250 mGy), an estimated lifetime excess of 19 (95% CI, 3-40) to 32 (95% CI, 5-66) solid cancer deaths could occur.
Conclusions and relevance: In RAI-treated patients with hyperthyroidism, greater organ-absorbed doses appeared to be modestly positively associated with risk of death from solid cancer, including breast cancer. Additional studies are needed of the risks and advantages of all major treatment options available to patients with hyperthyroidism.
Conflict of interest statement
Figures
Comment in
-
Letter to the editor: Use of radioactive iodine treatment in patients with hyperthyroidism? A case for shared decision making.Eur J Nucl Med Mol Imaging. 2019 Nov;46(12):2407. doi: 10.1007/s00259-019-04470-w. Epub 2019 Aug 3. Eur J Nucl Med Mol Imaging. 2019. PMID: 31375857 No abstract available.
-
Regarding the manuscript entitled "Association of Radioactive Iodine Treatment With Cancer Mortality in Patients With Hyperthyroidism".Eur J Nucl Med Mol Imaging. 2019 Nov;46(12):2410-2411. doi: 10.1007/s00259-019-04522-1. Epub 2019 Sep 6. Eur J Nucl Med Mol Imaging. 2019. PMID: 31492996 No abstract available.
-
Radioactive Iodine Treatment and Cancer Mortality in Hyperthyroid Patients: Questioning Standard Clinical Practice Requires Indisputable Scientific Data.J Nucl Med. 2019 Nov;60(11):1502-1503. doi: 10.2967/jnumed.119.234849. Epub 2019 Oct 4. J Nucl Med. 2019. PMID: 31586003 No abstract available.
-
There Is No Association of Radioactive Iodine Treatment with Cancer Mortality in Patients with Hyperthyroidism.J Nucl Med. 2019 Nov;60(11):1500-1501. doi: 10.2967/jnumed.119.235929. Epub 2019 Oct 4. J Nucl Med. 2019. PMID: 31586009 No abstract available.
-
Joint statement from the Society for Endocrinology and the British Thyroid Association regarding 'Association of Radioactive Iodine Treatment with cancer mortality in patients with hyperthyroidism'.Clin Endocrinol (Oxf). 2020 Mar;92(3):266-267. doi: 10.1111/cen.14136. Epub 2019 Dec 13. Clin Endocrinol (Oxf). 2020. PMID: 31788839 No abstract available.
-
Safety of the Use of Radioactive Iodine in Patients With Hyperthyroidism.JAMA Intern Med. 2019 Dec 1;179(12):1737-1738. doi: 10.1001/jamainternmed.2019.5117. JAMA Intern Med. 2019. PMID: 31790527 No abstract available.
-
Safety of the Use of Radioactive Iodine in Patients With Hyperthyroidism.JAMA Intern Med. 2019 Dec 1;179(12):1738-1739. doi: 10.1001/jamainternmed.2019.5120. JAMA Intern Med. 2019. PMID: 31790528 No abstract available.
-
Safety of the Use of Radioactive Iodine in Patients With Hyperthyroidism-Reply.JAMA Intern Med. 2019 Dec 1;179(12):1739. doi: 10.1001/jamainternmed.2019.5123. JAMA Intern Med. 2019. PMID: 31790535 Free PMC article. No abstract available.
-
Association of Radioactive Iodine Treatment of Hyperthyroidism With Cancer Mortality: An Unjustified Warning?J Clin Endocrinol Metab. 2020 Apr 1;105(4):dgz305. doi: 10.1210/clinem/dgz305. J Clin Endocrinol Metab. 2020. PMID: 31875905 No abstract available.
-
"Quid autem vides festucam in oculo fratris tui et trabem in oculo tuo non vide" on the hyperthyroidism-induced mortality and antithyroid drug-induced side effects in the era of radioiodine fake news.Eur J Nucl Med Mol Imaging. 2020 Jun;47(6):1342-1344. doi: 10.1007/s00259-020-04748-4. Eur J Nucl Med Mol Imaging. 2020. PMID: 32157430 No abstract available.
References
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
