

Risk factors for acute kidney injury in patients with acute myocardial infarction
- PMID: 31261199
- PMCID: PMC6759102
- DOI: 10.1097/CM9.0000000000000293
Risk factors for acute kidney injury in patients with acute myocardial infarction
Abstract
Background: Acute kidney injury (AKI) is a serious and fatal complication of acute myocardial infarction (AMI). It has high short- and long-term mortality rates and a poor prognosis but is potentially preventable. However, the current incidence, risk factors, and outcomes of AKI in the Chinese population are not well understood and would serve the first step to identify high-risk patients who could receive preventative care.
Methods: The medical data of 1124 hospitalized patients diagnosed with AMI from October 2013 to September 2015 were reviewed. AKI was defined according to the 2012 Kidney Disease Improving Global Outcomes criteria. All the patients were divided into either the AKI group or the non-AKI group. A univariate comparison analysis was performed to identify possible risk factors associated with AKI. A multiple logistic regression analysis was used to identify the independent risk factors for AKI in patients with AMI.
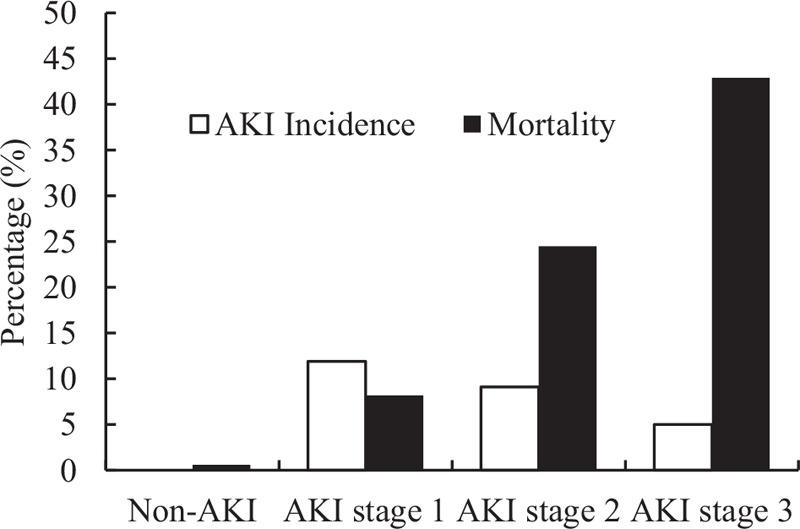
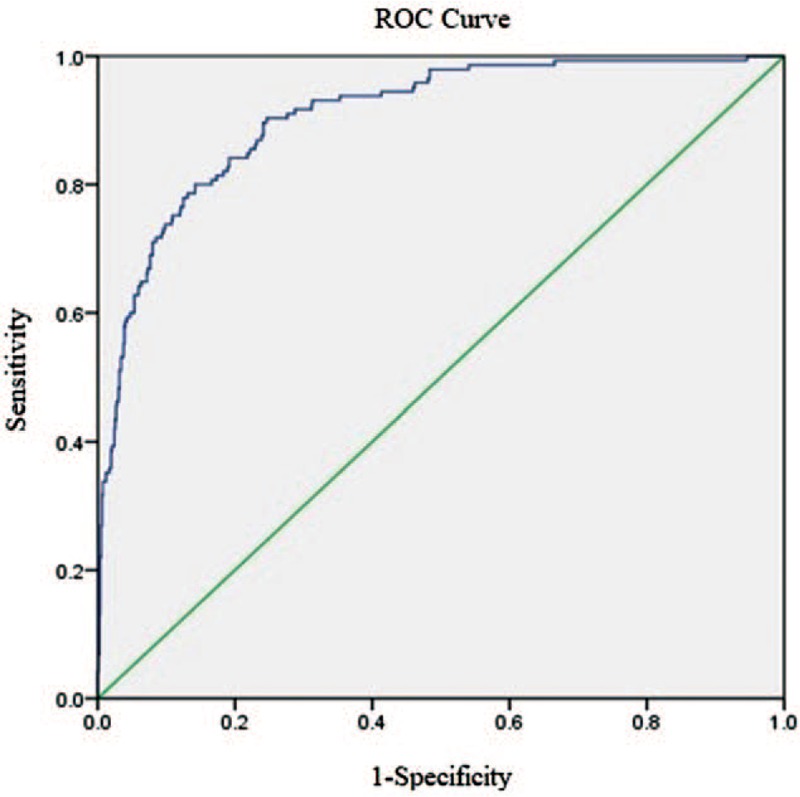
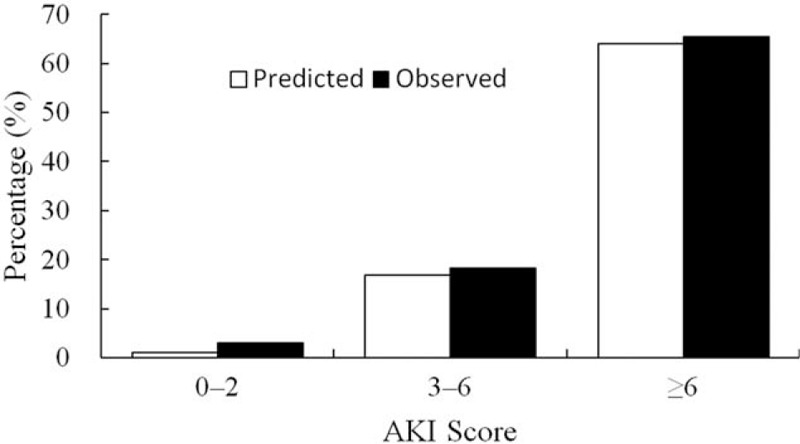
Results: Overall, the incidence of AKI was 26.0%. The mortality rate of the AKI group was 20.5%, and the mortality rate of the non-AKI group was 0.6% (P < 0.001). Logistic regression analysis showed that the independent risk factors for AKI in patients with AMI included: age (>60 years old) (odds ratio [OR] 1.04, 95% confidence interval [CI] 1.02-1.05, P = 0.000), hypertension (OR 2.51, 95% CI 1.62-3.87, P = 0.000), chronic kidney disease (OR 3.52, 95% CI 2.01-6.16, P = 0.000), Killip class ≥3 (OR 5.22, 95% CI 3.07-8.87, P = 0.000), extensive anterior myocardial infarction (OR 3.02, 95% CI 1.85-4.93, P = 0.000), use of furosemide (OR 1.02, 95% CI 1.02-1.03, P = 0.000), non-use of angiotensin-converting enzyme inhibitors/angiotensin receptor blocker (OR 1.58, 95% CI 1.04-2.40, P = 0.032). These factors provided an accurate tool to identify patients at high risk of developing AKI.
Conclusions: Approximately 26.0% of patients undergoing AMI developed AKI, and the development of AKI was strongly correlated with in-hospital mortality. The risk factors for AKI in patients with AMI were determined to help identify high-risk patients and make appropriate clinical decisions.
Figures
References
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol 2005; 16:3365–3370. doi: 10.1681/ASN.2004090740. - PubMed
-
- Yang L, Xing G, Wang L, Wu Y, Li S, Xu G, et al. Acute kidney injury in China: a cross-sectional survey. Lancet 2015; 386:1465–1471. doi: 10.1016/S0140-6736(15)00344-X. - PubMed
-
- Shacham Y, Leshem-Rubinow E, Steinvil A, Assa EB, Keren G, Roth A, et al. Renal impairment according to acute kidney injury network criteria among ST elevation myocardial infarction patients undergoing primary percutaneous intervention: a retrospective observational study. Clin Res Cardiol 2014; 103:525–532. doi: 10.1007/s00392-014-0680-8. - PubMed
-
- Tsai TT, Patel UD, Chang TI, Kennedy KF, Masoudi FA, Matheny ME, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR Cath-PCI registry. JACC Cardiovasc Interv 2014; 7:1–9. doi: 10.1016/j.jcin.2013.06.016. - PMC - PubMed
-
- Hwang SH, Jeong MH, Ahmed K, Kim MC, Cho KH, Lee MG, et al. Different clinical outcomes of acute kidney injury according to acute kidney injury network criteria in patients between ST elevation and non-ST elevation myocardial infarction. Int J Cardiol 2011; 150:99–101. doi: 10.1016/j.ijcard.2011.03.039. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
