

Fascia iliaca block in the emergency department for hip fracture: a randomized, controlled, double-blind trial
- PMID: 31262265
- PMCID: PMC6604210
- DOI: 10.1186/s12877-019-1193-0
Fascia iliaca block in the emergency department for hip fracture: a randomized, controlled, double-blind trial
Abstract
Background: Hip fracture causes moderate to severe pain and while fascia iliaca block has been reported to provide analgesic benefit, most previous trials were unblinded, with subsequent high risks of performance, selection and detection biases. In this randomized, control double-blind trial, we tested the hypothesis that a fascia iliaca block provides effective analgesia for patients suffering from hip fracture.
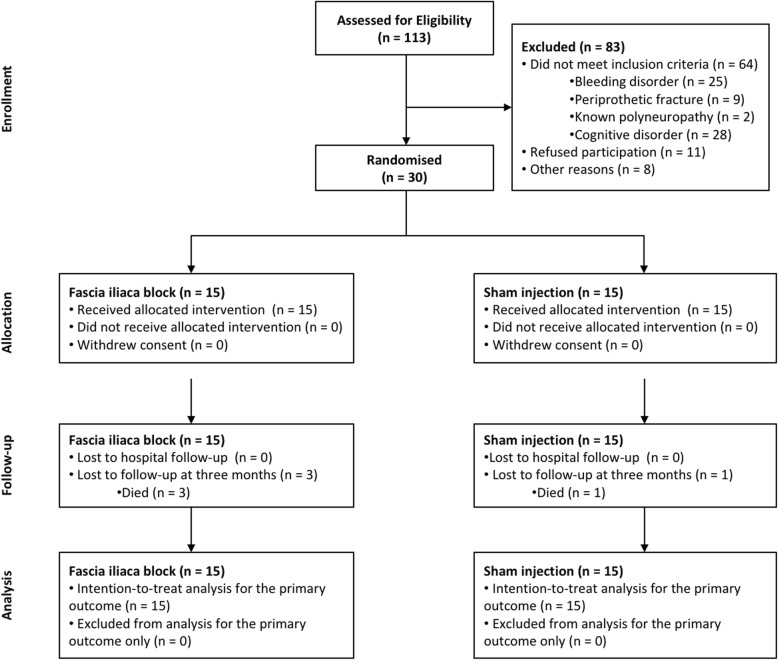
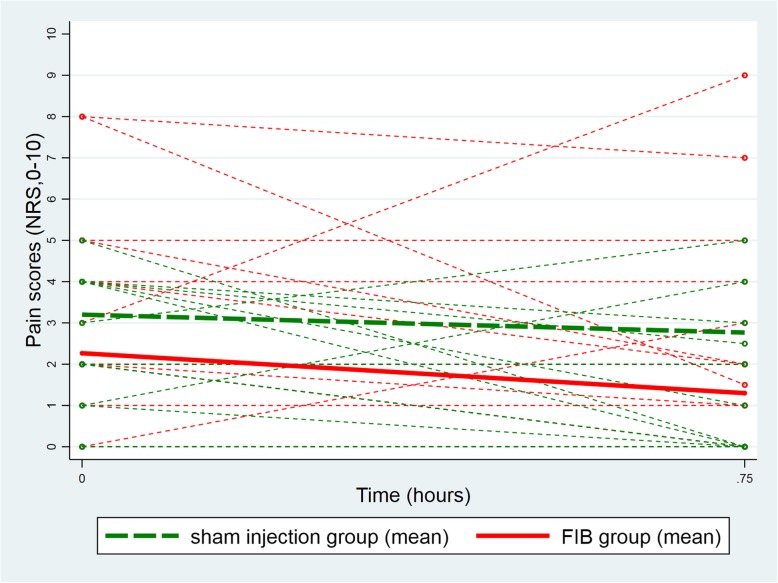
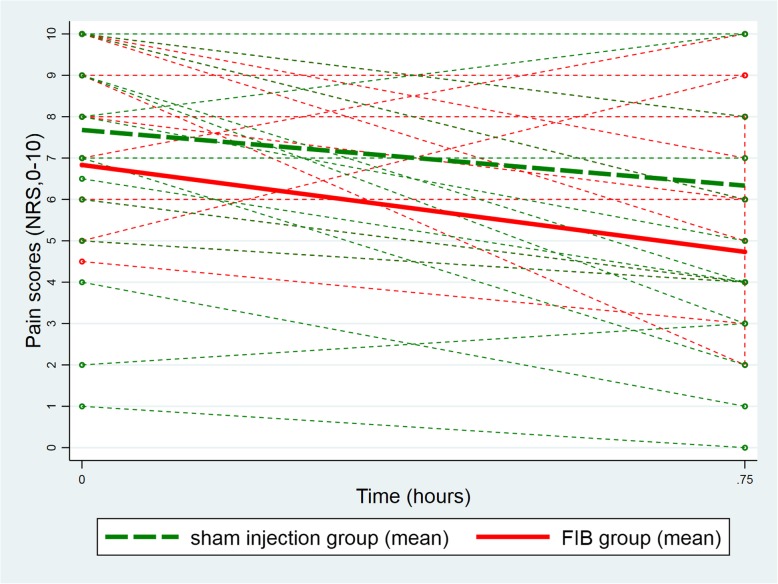
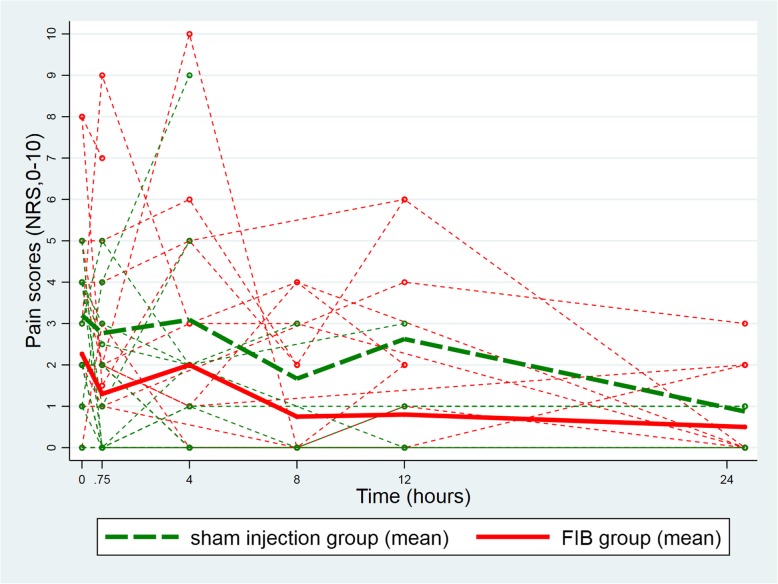
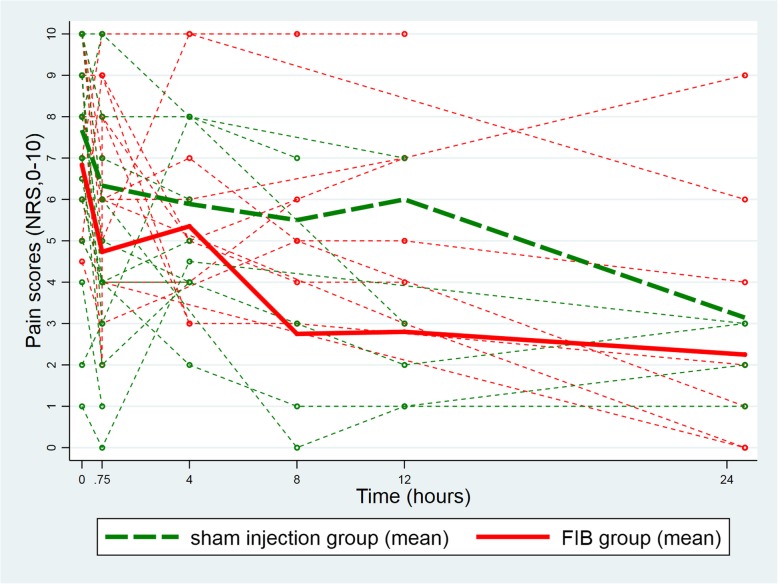
Methods: Thirty ASA I-III hip fracture patients over 70 years old, who received prehospital morphine, were randomized to receive either a fascia iliaca block using 30 ml of bupivacaine 0.5% with epinephrine 1:200,000 or a sham injection with normal saline. The fascia iliaca block was administered by emergency medicine physicians trained to perform an anatomic landmark-based technique. The primary outcome was the comparison between groups of the longitudinal pain score profiles at rest over the first 45 min following the procedure (numeric rating scale, 0-10). Secondary outcomes included the longitudinal pain score profiles on movement and the comparison over 4 h, 8 h, 12 h, and 24 h after the procedure, along with cumulative intravenous morphine consumption at 24 h.
Results: At baseline, the fascia iliaca group had a lower mean pain score than the sham injection group, both at rest (difference = - 0.9, 95%CI [- 2.4, 0.5]) and on movement (difference = - 0.9, 95%CI [- 2.7; 0.9]). These differences remained 45 min after the procedure and the two longitudinal pain score profiles were parallel both for patients at rest and on movement (test of parallelism for patients at rest p = 0.53 and on movement p = 0.45). The same parallel change in pain scores over time was observed over 24 h of follow-up (test of parallelism for patients at rest p = 0.82 and on movement p = 0.12). These results were confirmed after adjustment for gender, ASA score, and cumulative sums of intravenous morphine received pre-procedure and during-follow-up. In addition, there was no difference between the two groups in total cumulative intravenous morphine consumption at 24 h.
Conclusion: Fascia iliaca block following anatomic landmarks may not provide supplementary analgesia for patients suffering from hip fracture, when low pain scores are reported after prehospital morphine. Additional larger trials will help reach definitive conclusion.
Trial registration number: Clinicaltrials.gov - NCT02433548 . The study was registered retrospectively.
Keywords: Analgesia; Hip fractures; Lumbosacral plexus.
Conflict of interest statement
Dr. Eric Albrecht has received grants from the Swiss Academy for Anaesthesia Research (SACAR), Lausanne, Switzerland (50,000 CHF; no grant numbers attributed) and from B. Braun (Melsungen AG) to support his clinical research. EA has also received an honorarium from B. Braun Medical (Melsungen AG). No interest declared by the other authors.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
