

Ten year follow-up of lung transplantations using initially rejected donor lungs after reconditioning using ex vivo lung perfusion
- PMID: 31262311
- PMCID: PMC6604441
- DOI: 10.1186/s13019-019-0948-1
Ten year follow-up of lung transplantations using initially rejected donor lungs after reconditioning using ex vivo lung perfusion
Abstract
Background: In 2006 and 2007 we performed double lung transplantation with marginal donor lungs assessed and reconditioned by Ex Vivo Lung Perfusion (EVLP), using a technique developed by Professor Stig Steen. Here we present a 10-year follow-up comparing the outcomes of lung transplantations performed at our clinic using EVLP lungs vs. conventional lungs.
Method: Between 2006 and 2007, 21 patients (6 EVLP, 15 conventional) underwent double lung transplantation (LTx) with follow-up on May 2017 at Lund University Hospital, Sweden. Pulmonary function was measured at 3/6/12 months, and annually thereafter for a period of 10 years in addition to survival and freedom from chronic lung allograft dysfunction (CLAD) being analyzed.
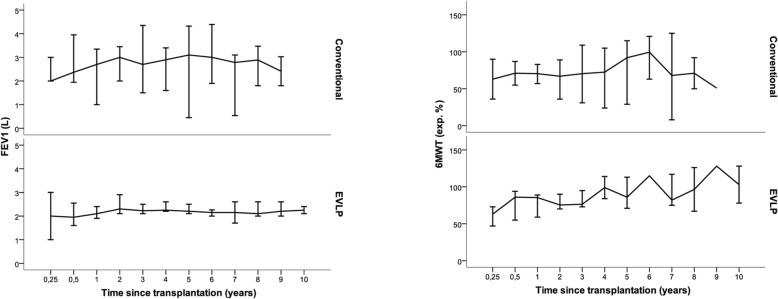
Results: Regarding Forced Expiratory Volume in 1 s (FEV1) and 6MWT at 3, 6, and 12 months and annually thereafter, no difference in median FEV1 nor 6MWT was found for EVLP-LTx vs. conventional-LTx (p > 0.05). No difference was shown in post-operative survival between EVLP-LTx vs. conventional LTx for patients with an overall survival up to 10-years (p > 0.05). The same pattern was shown in sub analyses for patients with a limited survival up to 1 and 5 years (p > 0.05).
Conclusion: No superiority was found in conventional-LTx over EVLP-LTx, neither in long-term survival nor pulmonary function. No difference in CLAD-free survival was seen between the two groups. We believe that EVLP is a safe and effective method to use in LTx, greatly increasing the donor pool by improving marginal lungs and providing an objective assessment of the viability of marginal donor lungs.
Keywords: EVLP; Long-term follow up; Lung function; Lung transplantation; Survival.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Kawut SM, Reyentovich A, Wilt JS, et al. Outcomes of extended donor lung recipients after lung transplantation. Transplantation. 2005;79:310–316. doi: 10.1097/01.TP.0000149504.53710.AE. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
