

Endoscopic management of gastric outlet obstruction disease
- PMID: 31263354
- PMCID: PMC6595925
- DOI: 10.20524/aog.2019.0390
Endoscopic management of gastric outlet obstruction disease
Abstract
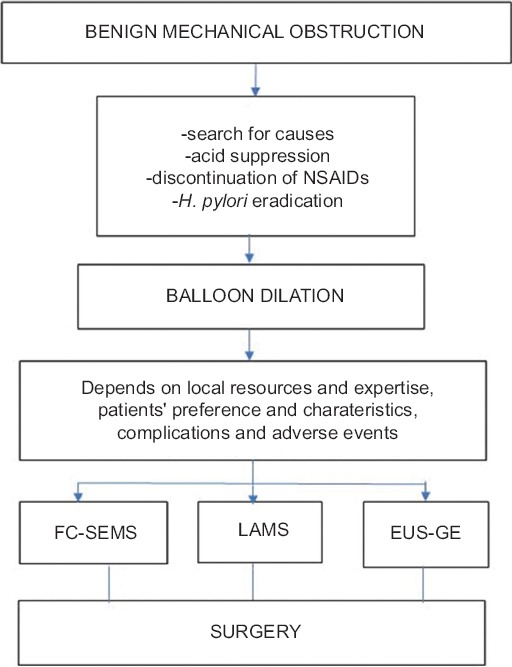
Gastric outlet obstruction (GOO) is a clinical syndrome characterized by a variety of symptoms. It may be caused by motor disorders and by benign or malignant mechanical disease. Endoscopic management of benign disease is mainly based on balloon dilation, augmented by the use of covered self-expanding metal stents (SEMS) in refractory disease. Endoscopic ultrasound-guided gastroenterostomy (EUS-GE) is increasingly used as an alternative method, although more studies with longer follow up are needed before it can be considered as a recommended therapy. Surgery remains the last resort. Endoscopic management of malignant GOO is based on SEMS placement as an alternative to palliative surgery, because it is a cost-effective method. The use of a covered or uncovered stent depends on patient-related variables, which include the stricture site, concomitant involvement of the bile duct, the patient's prognosis, probably the tumor type, and the use of chemotherapy. EUS-GE is a promising technique but needs more studies with longer follow up before any firm conclusions can be drawn.
Keywords: Gastric outlet obstruction disease; endoscopic balloon dilation; endoscopic ultrasound-guided gastroenterostomy; metal stents.
Conflict of interest statement
Conflict of Interest: None
Figures






References
-
- Johnson CD. Gastric outlet obstruction malignant until proved otherwise. Am J Gastroenterol. 1995;90:1740. - PubMed
-
- Shone DN, Nikoomanesh P, Smith-Meek MM, Bender JS. Malignancy is the most common cause of gastric outlet obstruction in the era of H2 blockers. Am J Gastroenterol. 1995;90:1769–1770. - PubMed
-
- Johnson CD, Ellis H. Gastric outlet obstruction now predicts malignancy. Br J Surg. 1990;77:1023–1024. - PubMed
-
- Chowdhury A, Dhali GK, Banerjee PK. Etiology of gastric outlet obstruction. Am J Gastroenterol. 1996;91:1679. - PubMed
-
- Cherian PT, Cherian S, Singh P. Long-term follow-up of patients with gastric outlet obstruction related to peptic ulcer disease treated with endoscopic balloon dilatation and drug therapy. Gastrointest Endosc. 2007;66:491–497. - PubMed
Publication types
LinkOut - more resources
Full Text Sources