

Clinical evaluation of the use of an mhealth intervention on quality of care provided by Community Health Workers in southwest Niger
- PMID: 31263555
- PMCID: PMC6594719
- DOI: 10.7189/jogh.09.010812
Clinical evaluation of the use of an mhealth intervention on quality of care provided by Community Health Workers in southwest Niger
Abstract
Background: Under the World Health Organization's (WHO) integrated community case management (iCCM) Rapid Access Expansion Program (RAcE), World Vision Niger and Canada supported the Niger Ministry of Public Health to implement iCCM in four health districts in Niger in 2013. Community health workers (CHWs), known as Relais Communautaire (RCom), were deployed in their communities to diagnose and treat children under five years of age presenting with diarrhea, malaria and pneumonia and refer children with severe illness to the higher-level facilities. Two of the districts in southwest Niger piloted RCom using smartphones equipped with an application to support quality case management and provide good timely clinical data. A two-arm cluster randomized trial assessed the impact of use of the mHealth application mainly on quality of care (QoC), but also on motivation, retention and supervision.
Methods: A two-arm cluster randomized trial was conducted from March to October 2016 in Dosso and Doutchi districts. The intervention arm comprised 66 RCom equipped with a smartphone and 64 in the paper-based control arm. Trained expert clinicians observed each RCom assessing sick children presenting to them (264 in intervention group; 256 in control group), re-assessed each child on the same set of parameters, and made further observations regarding perceptions of motivation, retention, supervision, drug management and caregiver satisfaction. The primary outcome was a QoC score composed of diagnostic and treatment variables. Other factors were assessed by questionnaires.
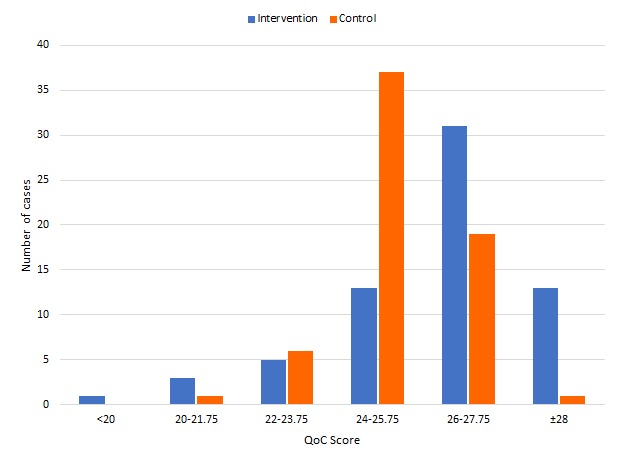
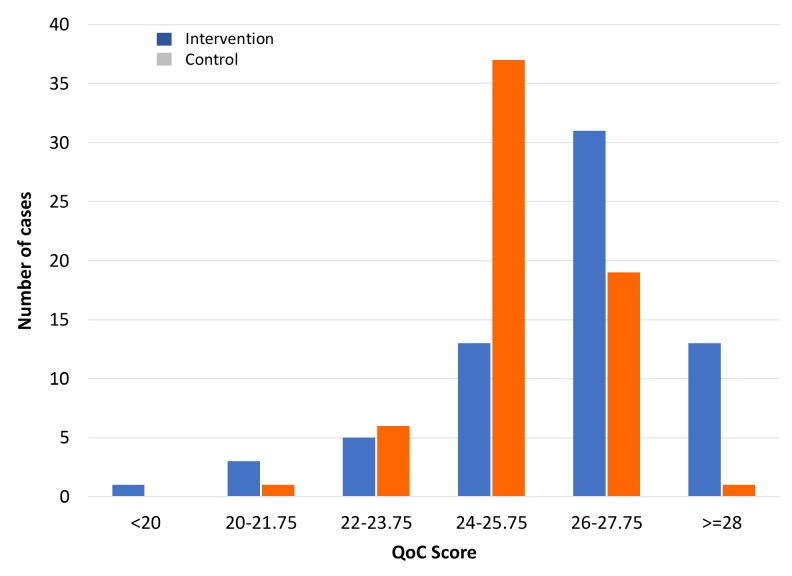
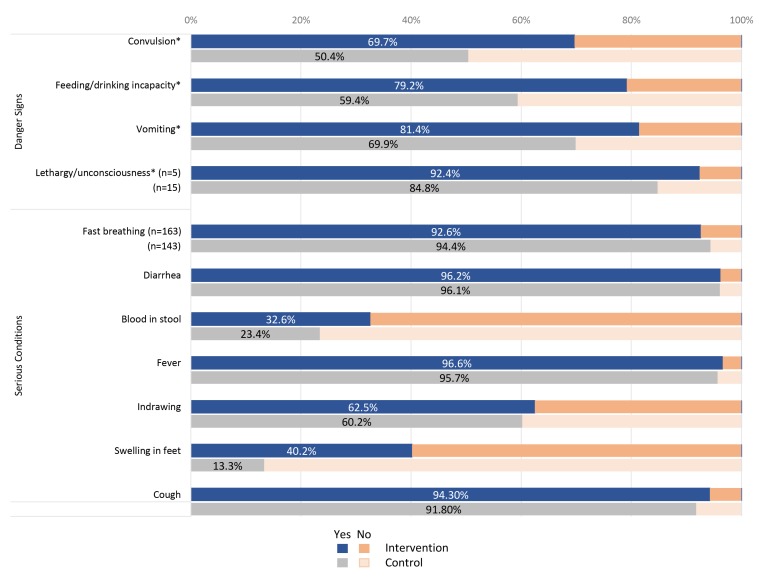
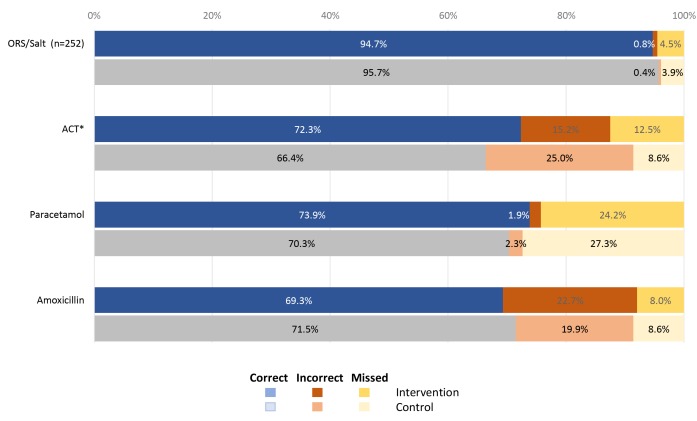
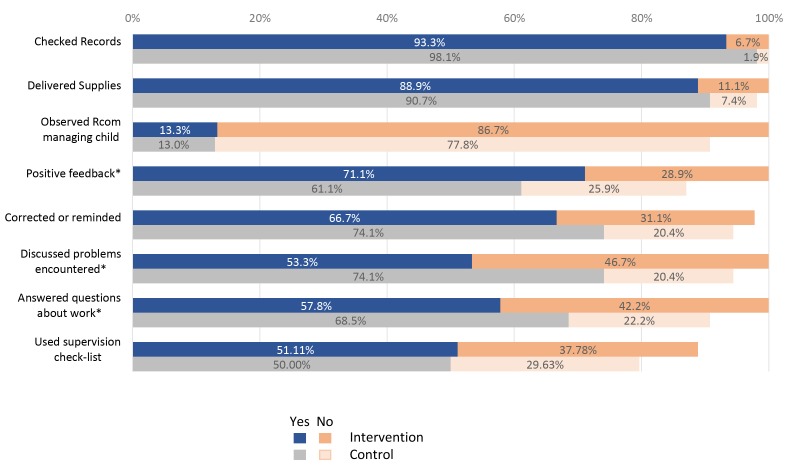
Results: On average, the mHealth equipped RCom showed a 3.4% higher QoC score (mean difference of 0.83 points). They were more likely to ask about the main danger signs: convulsions (69.7% vs 50.4%, P < 0.001); incapacity to drink or eat (79.2% vs 59.4%, P < 0.001); vomiting (81.4% vs 69.9%, P < 0.01); and lethargy or unconsciousness (92.4% vs 84.8%, P < 0.01). Specifically, they consistently asked one more screening question. They were also significantly better at examining for swelling feet (40.2% vs 13.3%, P < 0.01) and advising caretakers on diarrhea, drug dosage and administration, and performed (though non-significantly) better when examining cough and breathing rates, referring all conditions, getting children to take prescribed treatments immediately and having caregivers understand treatment continuation. The control group was significantly better at diagnosing fast breathing, bloody diarrhea and severe acute malnutrition; and was somewhat better (non-significant) at treating fever and malaria. With treatment in general of the three diseases, there was no significant difference between the groups. On further inspection, 83% of the intervention group had a QoC score greater than 80% (25 out of 31), whereas only 67% of the control group had comparable performance. With respect to referrals, the intervention group performed better, mostly based on their better assessment of danger signs, with more correct (85% vs 29%) and fewer missed, plus a lower proportion of incorrect referrals, with the reverse being true for the controls (P = 0.012). There were no statistically significant differences in motivation, retention and supervision between the two groups, yet intervention RCom reported double the rate of no supervision in the last three months (31.8% vs 15.6%).
Conclusions: Results suggest that use of the mHealth application led to modestly improved QoC through better assessment of the sick children and better referral decisions by RCom, but not to improvement in the actual treatment of malaria, pneumonia and diarrhea. Considering mHealth's additional costs and logistics, questions around its viability remain. Further implementation could be improved by investing in RCom capacity building, building organization culture and strengthened supervision, all essential areas for improving any CHW program. In this real-world setting, in poor and remote communities in rural Niger, this study did not support the overall value of the mHealth intervention. Much was learned for any future mHealth interventions and scale-up.
Conflict of interest statement
Competing interests: The authors completed the Unified Competing Interest form www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Figures
Similar articles
-
A mixed-methods quasi-experimental evaluation of a mobile health application and quality of care in the integrated community case management program in Malawi.J Glob Health. 2019 Jun;9(1):010811. doi: 10.7189/jogh.09.010811. J Glob Health. 2019. PMID: 31263554 Free PMC article.
-
Impact of mobile health-enhanced supportive supervision and supply chain management on appropriate integrated community case management of malaria, diarrhoea, and pneumonia in children 2-59 months: A cluster randomised trial in Eastern Province, Zambia.J Glob Health. 2020 Jun;10(1):010425. doi: 10.7189/jogh.10.010425. J Glob Health. 2020. PMID: 32509293 Free PMC article. Clinical Trial.
-
Effect of community-based intervention on improving access to treatment for sick under-five children in hard-to-reach communities in Niger State, Nigeria.J Glob Health. 2019 Jun;9(1):010803. doi: 10.7189/jogh.09.010803. J Glob Health. 2019. PMID: 31263548 Free PMC article.
-
Integrated community case management of childhood illness in low- and middle-income countries.Cochrane Database Syst Rev. 2021 Feb 10;2(2):CD012882. doi: 10.1002/14651858.CD012882.pub2. Cochrane Database Syst Rev. 2021. PMID: 33565123 Free PMC article.
-
Identifying and Treating Childhood Hearing Loss in Rural Alaska -- The Hearing Norton Sound Study [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2022 Feb. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2022 Feb. PMID: 39504398 Free Books & Documents. Review.
Cited by
-
Information and Communication Technology to Enhance the Implementation of the Integrated Management of Childhood Illness: A Systematic Review and Meta-Analysis.Mayo Clin Proc Digit Health. 2024 Jun 26;2(3):438-452. doi: 10.1016/j.mcpdig.2024.06.005. eCollection 2024 Sep. Mayo Clin Proc Digit Health. 2024. PMID: 40206116 Free PMC article. Review.
-
Systematic review of performance-enhancing health worker supervision approaches in low- and middle-income countries.Hum Resour Health. 2022 Jan 6;20(1):2. doi: 10.1186/s12960-021-00692-y. Hum Resour Health. 2022. PMID: 34991604 Free PMC article.
-
Long-term quality of integrated community case management care for children in Bugoye Subcounty, Uganda: a retrospective observational study.BMJ Open. 2022 Apr 22;12(4):e051015. doi: 10.1136/bmjopen-2021-051015. BMJ Open. 2022. PMID: 35459661 Free PMC article.
-
Cross-cultural adaptation and psychometric properties of the Herth Hope Index in Kinyarwanda: adapting a positive psychosocial tool for healthcare recipients and providers in the Rwandan setting.Health Qual Life Outcomes. 2020 Aug 24;18(1):286. doi: 10.1186/s12955-020-01537-3. Health Qual Life Outcomes. 2020. PMID: 32831084 Free PMC article.
-
Improving community health worker treatment for malaria, diarrhoea, and pneumonia in Uganda through inSCALE community and mHealth innovations: A cluster randomised controlled trial.PLOS Digit Health. 2023 Jun 12;2(6):e0000217. doi: 10.1371/journal.pdig.0000217. eCollection 2023 Jun. PLOS Digit Health. 2023. PMID: 37307519 Free PMC article.
References
-
- United Nations Development Programme. Human Development Report 2016: Human development for everyone, p. 25. Available: http://hdr.undp.org/sites/default/files/HDR2016_EN_Overview_Web.pdf. Accessed: 28 February 2019.
-
- The World Bank Data. Fertility rate, total (births per woman). Available: https://data.worldbank.org/indicator/SP.DYN.TFRT.IN. Accessed: 28 February 2019.
-
- UNICEF Data. Monitoring the situation of children and women. United Nations Inter-agency Group for Child Mortality Estimation (UN IGME), 2017. Available: https://data.unicef.org. Accessed: 28 February 2019.
-
- UNICEF Data. Child Survival, Under-five mortality, March 2018. Available: https://data.unicef.org/topic/child-survival/under-five-mortality/. Accessed: 28 February 2019.
-
- World Health Organization /UNICEF Joint Statement on Integrated Community Case Management: An equity-focused strategy to improve access to essential treatment services for children, June 2012. Available: https://www.unicef.org/health/files/iCCM_Joint_Statement_2012.pdf. Accessed: 28 February 2019. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
