

The Clinical Rationale for the Sentry Bioconvertible Inferior Vena Cava Filter for the Prevention of Pulmonary Embolism
- PMID: 31263598
- PMCID: PMC6556320
- DOI: 10.1155/2019/5795148
The Clinical Rationale for the Sentry Bioconvertible Inferior Vena Cava Filter for the Prevention of Pulmonary Embolism
Abstract
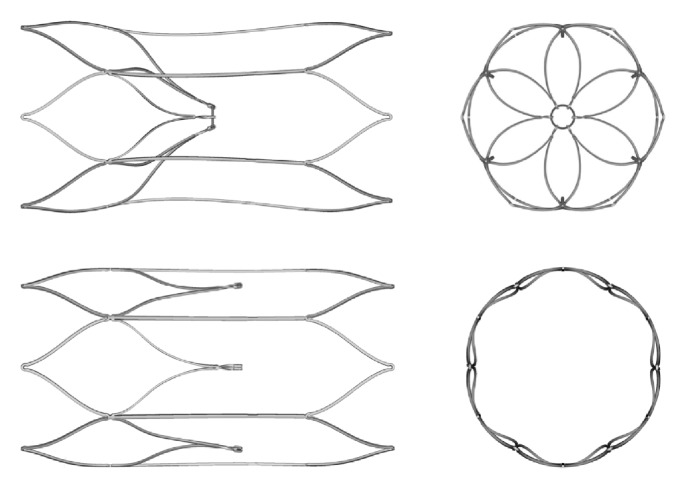
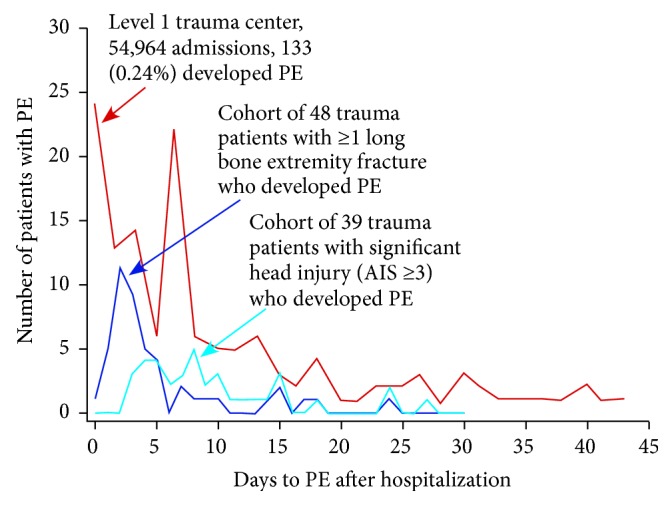
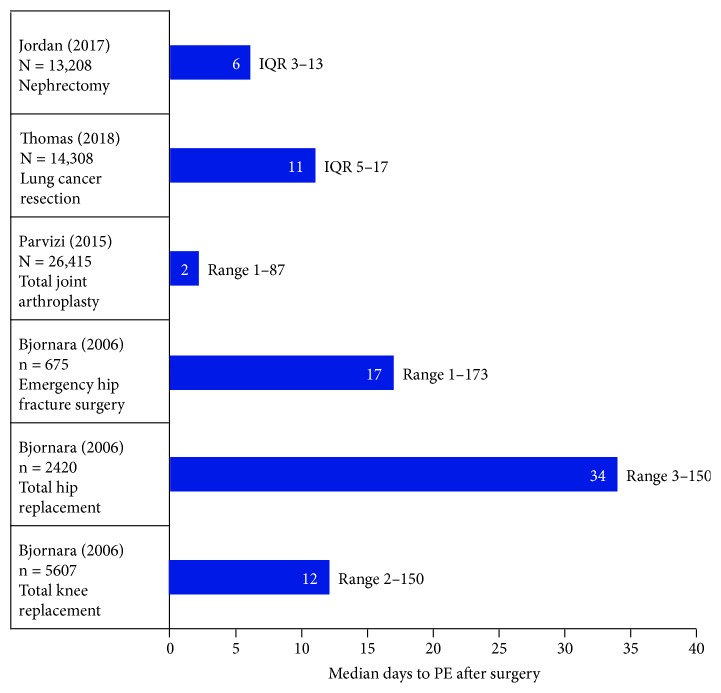
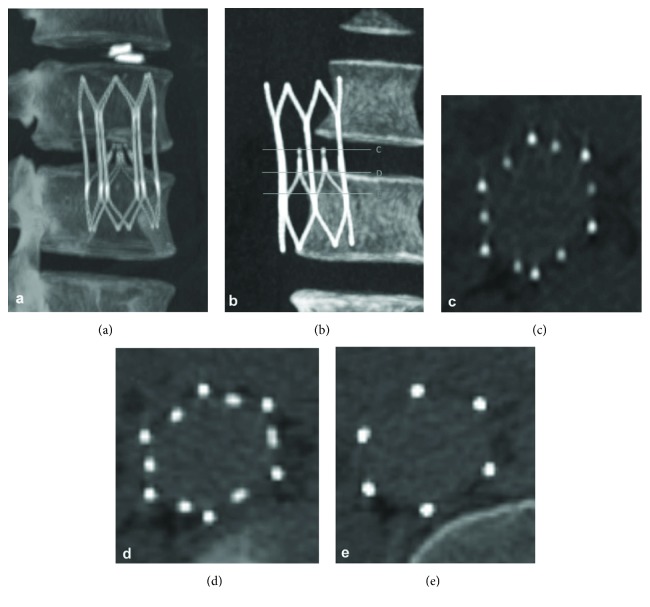
The Sentry inferior vena cava (IVC) filter is designed to provide temporary protection against pulmonary embolism (PE) during transient high-risk periods and then to bioconvert after 60 days after implantation. At the time of bioconversion, the device's nitinol arms retract from the filtering position into the caval wall. Subsequently, the stable stent-like nitinol frame is endothelialized. The Sentry bioconvertible IVC filter has been evaluated in a multicenter investigational-device-exemption pivotal trial (NCT01975090) of 129 patients with documented deep vein thrombosis (DVT) or PE, or at temporary risk of developing DVT or PE, and with contraindications to anticoagulation. Successful filter conversion was observed in 95.7% of patients at 6 months (110/115) and 96.4% at 12 months (106/110). Through 12 months, there were no cases of symptomatic PE. The rationale for development of the Sentry bioconvertible device includes the following considerations: (1) the period of highest risk of PE for the vast majority of patients occurs within the first 60 days after an index event, with most of the PEs occurring in the first 30 days; (2) the design of retrievable IVC filters to support their removal after a transitory high-PE-risk period has, in practice, been associated with insecure filter dynamics and time-dependent complications including tilting, fracture, embolization, migration, and IVC perforation; (3) most retrievable IVC filters are placed for temporary protection, but for a variety of reasons they are not removed in any more than half of implanted patients, and when removal is attempted, the procedure is not always successful even with advanced techniques; and (4) analysis of Medicare hospital data suggests that payment for the retrieval procedure does not routinely compensate for expense. The Sentry device is not intended for removal after bioconversion. In initial clinical use, complications have been limited. Long-term results for the Sentry bioconvertible IVC filter are anticipated soon.
Figures
References
-
- Guyatt G. H., Akl E. A., Crowther M., Gutterman D. D., Schünemann H. J. Executive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2):7S–47S. doi: 10.1378/chest.1412S3. - DOI - PMC - PubMed
-
- ACR-SIR-SPR Practice Parameter for the Performance of Inferior Vena Cava (IVC) Filter Placement for the Prevention of Pulmonary Embolism. 2016. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/ivc-fliterplac.... - PubMed
Publication types
LinkOut - more resources
Full Text Sources
