

Timing and magnitude of regional right ventricular function and their relationship with early hospital mortality in patients with acute pulmonary embolism
- PMID: 31264657
- PMCID: PMC6683210
- DOI: 10.14744/AnatolJCardiol.2019.38906
Timing and magnitude of regional right ventricular function and their relationship with early hospital mortality in patients with acute pulmonary embolism
Abstract
Objective: Right ventricular (RV) dysfunction in acute pulmonary embolism (APE) has been associated with increased mortality and morbidity. The aim of the present study was to assess the timing and magnitude of regional RV functions using speckle-tracking echocardiography (STE) and their relationship to early hospital mortality in patients with APE.
Methods: One hundred forty-two patients were prospectively studied at the onset of an acute episode and after a median follow-up period of 30 days. Their clinical and laboratory characteristics were recorded. For all patients, conventional two-dimensional echocardiography and STE were performed within 24 h after the diagnosis of APE.
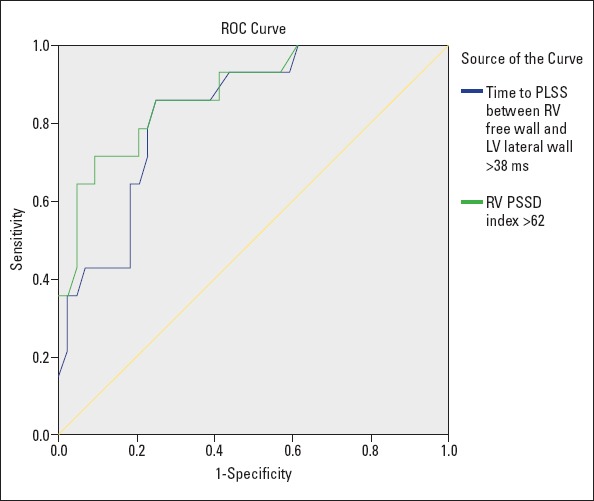
Results: Twenty-eight (19.7%) patients died during the hospitalization follow-up. Patients who died during hospitalization were older and had higher high sensitivity cardiac troponin T levels, and a higher percentage of patients had simplified Pulmonary Embolism Severity Indexes. In STE analyses, they had lower RV free wall peak longitudinal systolic strain (PLSS) and higher RV peak systolic strain dispersion indexes. The time to PLSS difference between RV free wall and LV lateral was longer in patients who died during hospitalization than in those who survived, and this was an independent predictor of early hospital mortality with 85.7% sensitivity and 75.0% specificity in patients with APE.
Conclusion: APE was associated with RV electromechanical delay and dispersion. Electromechanical delay index might be useful to predict early hospital mortality in patients with APE.
Conflict of interest statement
Figures
Similar articles
-
Assessment of right ventricular function and relation to mortality after acute pulmonary embolism: A speckle tracking echocardiography-based study.Echocardiography. 2019 Jul;36(7):1298-1305. doi: 10.1111/echo.14398. Epub 2019 Jun 11. Echocardiography. 2019. PMID: 31184782
-
Right ventricular function in acute pulmonary embolism: a combined assessment by three-dimensional and speckle-tracking echocardiography.J Am Soc Echocardiogr. 2014 Mar;27(3):329-38. doi: 10.1016/j.echo.2013.11.013. Epub 2013 Dec 8. J Am Soc Echocardiogr. 2014. PMID: 24325961
-
Prognostic value of echocardiographic parameters for right ventricular function in patients with acute non-massive pulmonary embolism.Heart Vessels. 2019 Jul;34(7):1187-1195. doi: 10.1007/s00380-019-01340-1. Epub 2019 Jan 22. Heart Vessels. 2019. PMID: 30671642
-
ST-segment elevation in V1-V4 in acute pulmonary embolism: a case presentation and review of literature.Eur Heart J Acute Cardiovasc Care. 2016 Dec;5(8):579-586. doi: 10.1177/2048872615604273. Epub 2015 Sep 15. Eur Heart J Acute Cardiovasc Care. 2016. PMID: 26373811 Review.
-
The Role of Troponin in the Diagnosis and Treatment of Acute Pulmonary Embolism: Mechanisms of Elevation, Prognostic Evaluation, and Clinical Decision-Making.Cureus. 2024 Aug 27;16(8):e67922. doi: 10.7759/cureus.67922. eCollection 2024 Aug. Cureus. 2024. PMID: 39328637 Free PMC article. Review.
Cited by
-
Elevated D-Dimers and Right Ventricular Dysfunction on Echocardiography for Diagnosis of Pulmonary Embolism: A Validation Study.Cureus. 2020 Oct 3;12(10):e10778. doi: 10.7759/cureus.10778. Cureus. 2020. PMID: 33154846 Free PMC article.
-
Prognostic role of different findings at echocardiography in acute pulmonary embolism: a critical review and meta-analysis.ERJ Open Res. 2023 Mar 27;9(2):00641-2022. doi: 10.1183/23120541.00641-2022. eCollection 2023 Mar. ERJ Open Res. 2023. PMID: 37009027 Free PMC article.
References
-
- Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35:3033–69. - PubMed
-
- Mayo J, Thakur Y. Acute pulmonary embolism:from morphology to function. Semin Respir Crit Care Med. 2014;35:41–9. - PubMed
-
- Becattini C, Agnelli G. Predictors of mortality from pulmonary embolism and their influence on clinical management. Thromb Haemost. 2008;100:747–51. - PubMed
-
- Angriman F, Vazquez FJ, Roy PM, Le Gal G, Carrier M, Gandara E. A new prognostic strategy for adult patients with acute pulmonary embolism eligible for outpatient therapy. J Thromb Thrombolysis. 2017;43:326–32. - PubMed
-
- Grifoni S, Olivotto I, Cecchini P, Pieralli F, Camaiti A, Santoro G, et al. Short-term clinical outcome of patients with acute pulmonary embolism, normal blood pressure, and echocardiographic right ventricular dysfunction. Circulation. 2000;101:2817–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
