

Mobile telephone-delivered contingency management interventions promoting behaviour change in individuals with substance use disorders: a meta-analysis
- PMID: 31265747
- PMCID: PMC6852192
- DOI: 10.1111/add.14725
Mobile telephone-delivered contingency management interventions promoting behaviour change in individuals with substance use disorders: a meta-analysis
Abstract
Background/aims: Contingency management (CM) interventions have gained considerable interest due to their success in the treatment of addiction. However, their implementation can be resource-intensive for clinical staff. Mobile telephone-based systems might offer a low-cost alternative. This approach could facilitate remote monitoring of behaviour and delivery of the reinforcer and minimize issues of staffing and resources. This systematic review and meta-analysis assessed the evidence for the effectiveness of mobile telephone-delivered CM interventions to promote abstinence (from drugs, alcohol and tobacco), medication adherence and treatment engagement among individuals with substance use disorders.
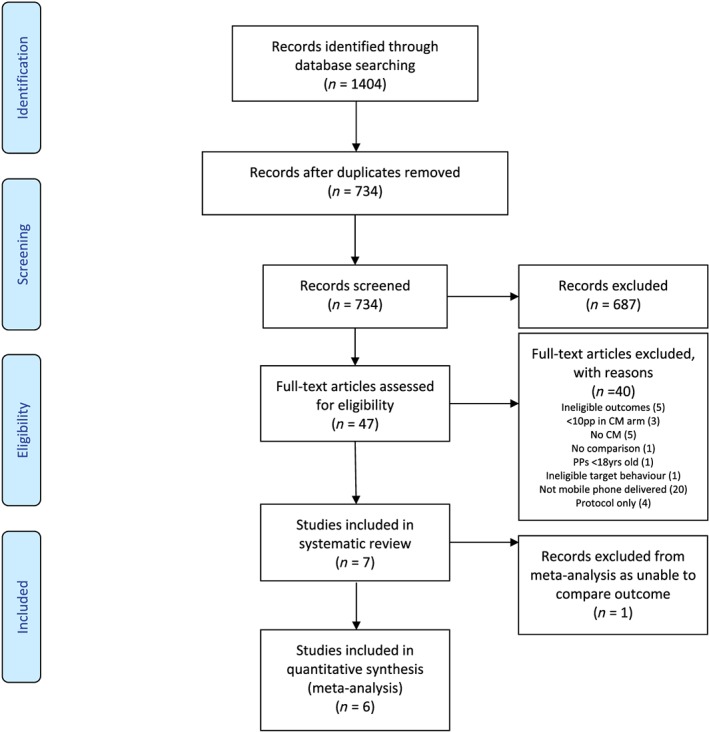
Design: A systematic search of databases (PsychINFO, CINAHL, MEDLINE PubMed, CENTRAL, Embase) for randomized controlled trials and within-subject design studies (1995-2019). The review was conducted in accordance with the PRISMA statement. The protocol was registered on PROSPERO.
Setting: All included studies originated in the United states.
Participants: Seven studies were found, including 222 participants; two targeted alcohol abstinence among frequent drinkers and four targeted smoking cessation (in homeless veterans and those with post-traumatic stress disorder). One targeted medication adherence.
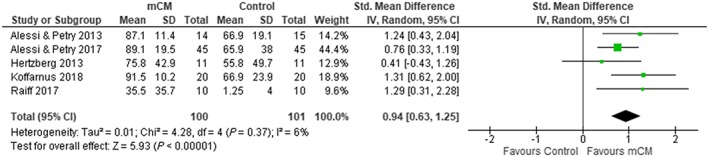
Measures: The efficacy of CM to increase alcohol and nicotine abstinence was compared with control using several outcomes; percentage of negative samples (PNS), quit rate (QR) and longest duration abstinent (LDA) at the end of the intervention.
Findings: The random-effects meta-analyses produced pooled effect sizes of; PNS [d = 0.94, 95% confidence interval (CI) = 0.63-1.25], LDA (d = 1.08, 95% CI = 0.69-1.46) and QR (d = 0.46, 95% CI = 0.27-0.66), demonstrating better outcomes across the CM conditions. Most of the studies were rated as of moderate quality. 'Fail-safe N' computations for PNS indicated that 50 studies would be needed to produce a non-significant overall effect size. None could be calculated for QR and LDA due to insufficient number of studies.
Conclusion: Mobile telephone-delivered contingency management performs significantly better than control conditions in reducing tobacco and alcohol use among adults not in treatment for substance use disorders.
Keywords: Contingency management; drug use; financial incentives; mobile telephone; remote monitoring; substance use.
© 2019 The Authors. Addiction published by John Wiley & Sons Ltd on behalf of Society for the Study of Addiction.
Figures


References
-
- Prendergast M., Podus D., Finney J., Greenwell L., Roll J. Contingency management for treatment of substance use disorders: a meta‐analysis. Addiction 2006; 101: 1546–1560. - PubMed
-
- Lussier J. P., Heil S. H., Mongeon J. A., Badger G. J., Higgins S. T. A meta‐analysis of voucher‐based reinforcement therapy for substance use disorders. Addiction 2006; 101: 192–203. - PubMed
-
- Griffith J. D., Rowan‐Szal G. A., Roark R. R., Simpson D. D. Contingency management in outpatient methadone treatment: a meta‐analysis. Drug Alcohol Depend 2000; 58: 55–66. - PubMed
-
- Higgins S. T., Silverman K. Contingency Management in Substance Abuse Treatment. New York, NY: Guilford Press; 2008.
