

Urgent-start peritoneal dialysis for patients with end stage renal disease: a 10-year retrospective study
- PMID: 31266466
- PMCID: PMC6604308
- DOI: 10.1186/s12882-019-1408-9
Urgent-start peritoneal dialysis for patients with end stage renal disease: a 10-year retrospective study
Abstract
Background: Urgent-start peritoneal dialysis (PD) can help patients with end-stage renal diseases (ESRD) that are referred late to dialysis. However, catheter patency and related complications of urgent-start PD have not been thoroughly clarified. We investigated the clinical outcomes of urgent-start PD in a Chinese cohort.
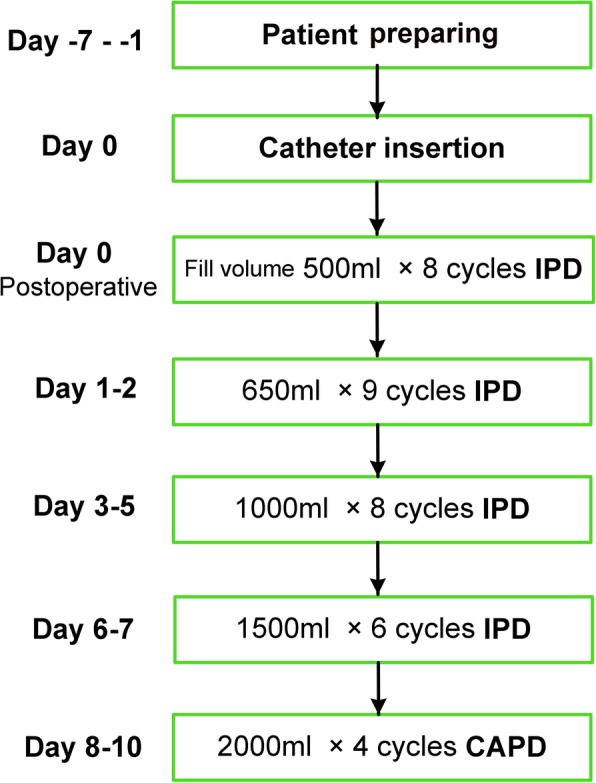
Methods: We enrolled ESRD patients who received urgent-start PD (starting PD within 14 days after catheter insertion) in our center from January 1, 2006 to December 31, 2014, and followed them up for 10 years. The primary outcome was catheter failure. Secondary outcomes included short-term and long-term complications related to urgent-start PD.
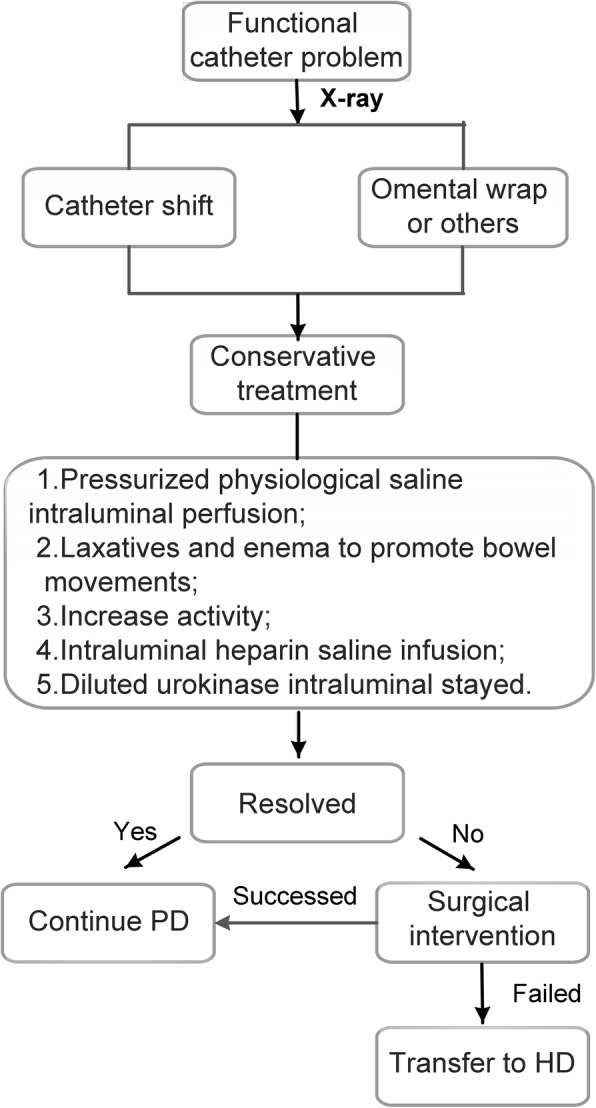
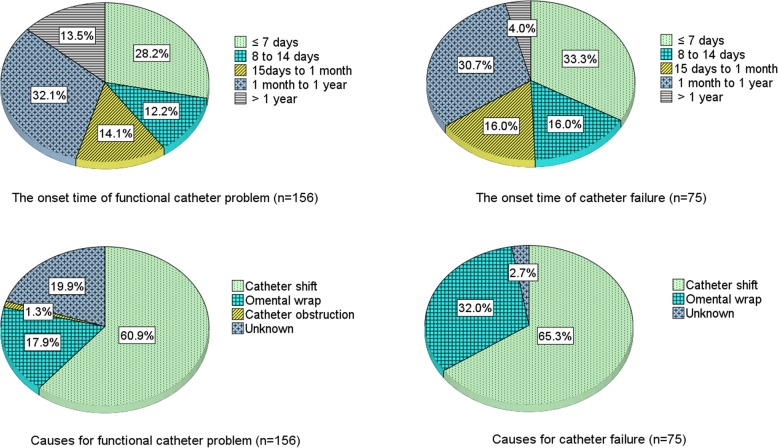
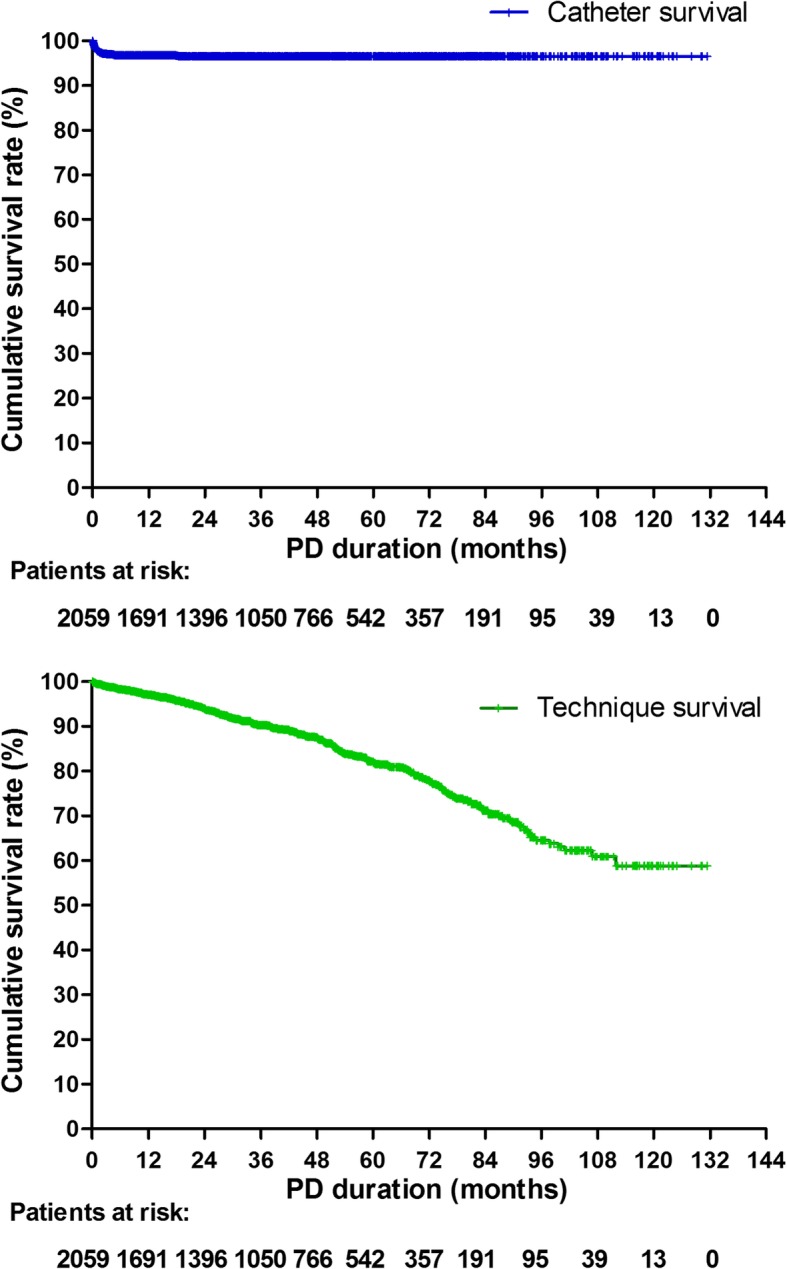
Results: Totally 2059 patients (58.9% male, mean age 47.6 ± 15.9 years) were enrolled. Few perioperative complications were observed, including significant hemorrhage (n = 3, 0.1%) and bowel perforation (n = 0). Early peritonitis occurred in 24 (1.2%) patients (0.28 episodes per patient-year). Within the first month after catheter insertion, functional catheter malfunction occurred in 85 (4.1%) patients, and abdominal wall complications (including hernia, hydrothorax, hydrocele, and leakage) in 36 (1.7%) patients. During a median 36.5 (17.7-61.4) months of follow-up, 75 (3.6%) patients experienced catheter failure, and 291 (14.1%) had death-censoring technique failure. At the end of 1-month, 1 -year, 3-year, and 5-year, catheter patency rate was 97.6, 96.4, 96.2, 96.2%; and technique survival rate was 99.5, 97.0, 90.3, 82.7%, respectively. After adjusting for confounders, every 5-year increase in age was associated with 19% decrease of risk for catheter failure (hazard ratio [HR]: 0.81, 95% confidence interval [CI]: 0.73-0.89). Male sex (HR: 1.43, 95% CI: 1.00-2.04), diabetic nephropathy (HR: 1.56, 95% CI: 1.08-2.25) and low hemoglobin levels (HR: 0.89, 95% CI: 0.81-0.98) were independent risk factors for abdominal wall complications.
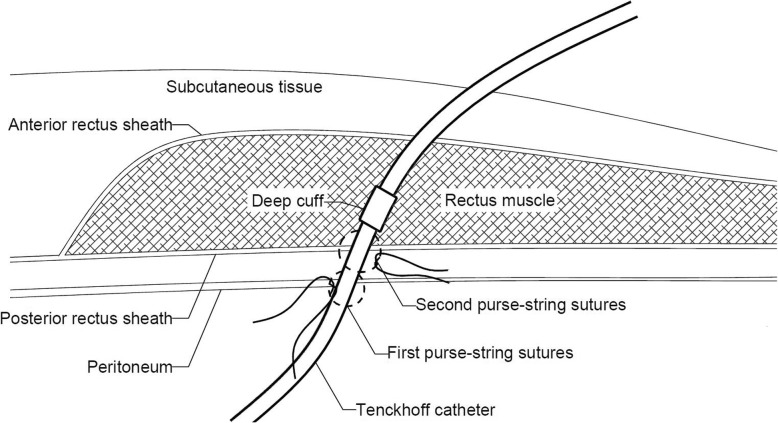
Conclusions: Urgent-start PD is a safe and efficacious option for unplanned ESRD patients. A well-trained PD team, a standardized catheter insertion procedure by experienced nephrologists, and a carefully designed initial PD prescription as well as comprehensive follow-up care, might be essential for the successful urgent-start PD program.
Keywords: Catheter patency; Complications; End stage renal disease; Peritoneal dialysis; Technique survival; Urgent-start peritoneal dialysis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Urgent start peritoneal dialysis: are we there yet?BMC Nephrol. 2020 Jan 31;21(1):39. doi: 10.1186/s12882-020-1706-2. BMC Nephrol. 2020. PMID: 32005195 Free PMC article.
References
-
- United States Renal Data System . 2017 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2017.
-
- Yu X. How to set up PD centres: the Chinese perspective. 2017. http://www.thelancet.com/campaigns/kidney/updates. Accessed May 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
