

The reproducibility of psychiatric evaluations of work disability: two reliability and agreement studies
- PMID: 31266488
- PMCID: PMC6607597
- DOI: 10.1186/s12888-019-2171-y
The reproducibility of psychiatric evaluations of work disability: two reliability and agreement studies
Abstract
Background: Expert psychiatrists conducting work disability evaluations often disagree on work capacity (WC) when assessing the same patient. More structured and standardised evaluations focusing on function could improve agreement. The RELY studies aimed to establish the inter-rater reproducibility (reliability and agreement) of 'functional evaluations' in patients with mental disorders applying for disability benefits and to compare the effect of limited versus intensive expert training on reproducibility.
Methods: We performed two multi-centre reproducibility studies on standardised functional WC evaluation (RELY 1 and 2). Trained psychiatrists interviewed 30 and 40 patients respectively and determined WC using the Instrument for Functional Assessment in Psychiatry (IFAP). Three psychiatrists per patient estimated WC from videotaped evaluations. We analysed reliability (intraclass correlation coefficients [ICC]) and agreement ('standard error of measurement' [SEM] and proportions of comparisons within prespecified limits) between expert evaluations of WC. Our primary outcome was WC in alternative work (WCalternative.work), 100-0%. Secondary outcomes were WC in last job (WClast.job), 100-0%; patients' perceived fairness of the evaluation, 10-0, higher is better; usefulness to psychiatrists.
Results: Inter-rater reliability for WCalternative.work was fair in RELY 1 (ICC 0.43; 95%CI 0.22-0.60) and RELY 2 (ICC 0.44; 0.25-0.59). Agreement was low in both studies, the 'standard error of measurement' for WCalternative.work was 24.6 percentage points (20.9-28.4) and 19.4 (16.9-22.0) respectively. Using a 'maximum acceptable difference' of 25 percentage points WCalternative.work between two experts, 61.6% of comparisons in RELY 1, and 73.6% of comparisons in RELY 2 fell within these limits. Post-hoc secondary analysis for RELY 2 versus RELY 1 showed a significant change in SEMalternative.work (- 5.2 percentage points WCalternative.work [95%CI - 9.7 to - 0.6]), and in the proportions on the differences ≤ 25 percentage points WCalternative.work between two experts (p = 0.008). Patients perceived the functional evaluation as fair (RELY 1: mean 8.0; RELY 2: 9.4), psychiatrists as useful.
Conclusions: Evidence from non-randomised studies suggests that intensive training in functional evaluation may increase agreement on WC between experts, but fell short to reach stakeholders' expectations. It did not alter reliability. Isolated efforts in training psychiatrists may not suffice to reach the expected level of agreement. A societal discussion about achievable goals and readiness to consider procedural changes in WC evaluations may deserve considerations.
Keywords: Disability evaluation; Evidence-based medicine; Observer variation; Reproducibility of results; Return to work; Social security; Work capacity evaluation.
Conflict of interest statement
None of the authors received support from any external organization or company for the submitted work. No financial relationships with any organizations that might have an interest in the submitted work in the previous three years; after data collection was finished (07/2016), RK became head of the Medical Competence Center of Suva, Lucerne. No other relationships or activities that could appear to have influenced the submitted work.
Figures
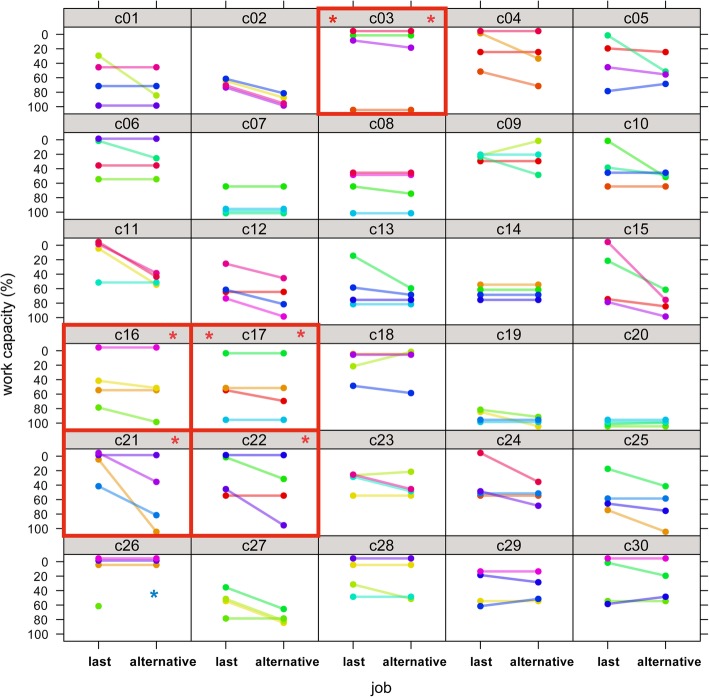
 Patients with maximum divergent expert ratings.
Patients with maximum divergent expert ratings.  For ‘alternative work’, one rating of patient 26 was excluded from the analysis due to a violation of the rating rules
For ‘alternative work’, one rating of patient 26 was excluded from the analysis due to a violation of the rating rules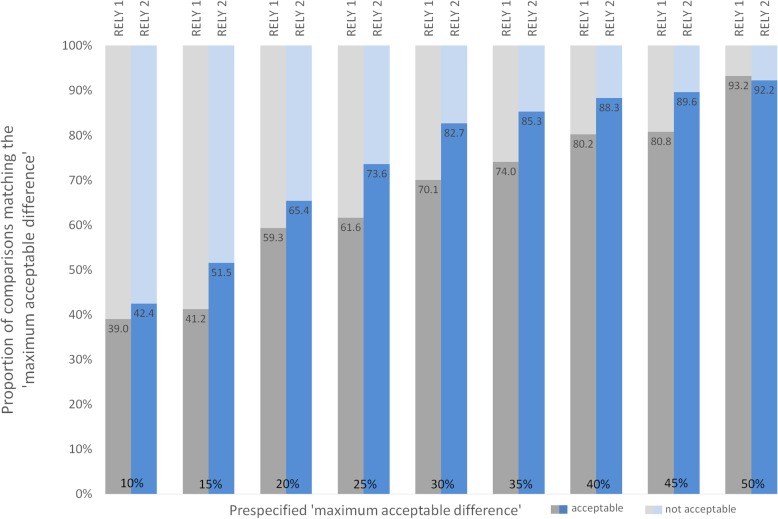
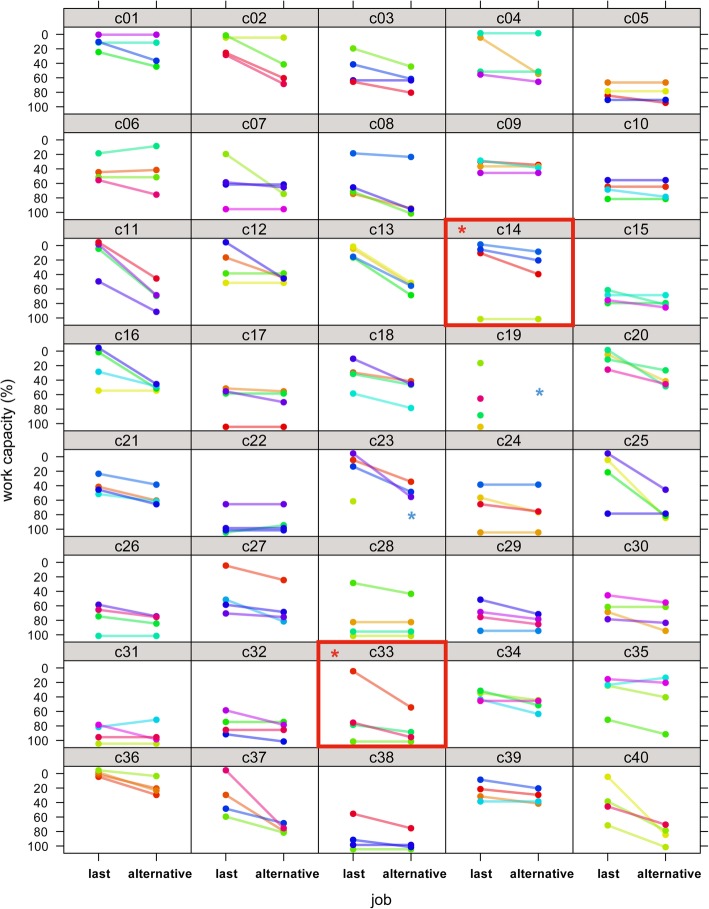
 Patients with maximum divergent ratings.
Patients with maximum divergent ratings.  For ‘alternative work’, all ratings of patient 19 and one rating of patient 23 were excluded from the analysis due to violations of the rating rules
For ‘alternative work’, all ratings of patient 19 and one rating of patient 23 were excluded from the analysis due to violations of the rating rulesReferences
-
- International Social Security Association I: Country Profiles. https://www.issa.int/en/country-profiles, last accessed 14.04.2019.
-
- OECD . Sickness, disability and work: breaking the barriers. A synthesis of findings across OECD countries. Paris: OECD; 2010.
-
- Schandelmaier S, Fischer K, Mager R, Hoffmann-Richter U, Leibold A, Bachmann MS, Kedzia S, Jeger J, Marelli R, Kunz R, et al. Evaluation of work capacity in Switzerland: a survey among psychiatrists about practice and problems. Swiss Med Wkly. 2013;143:w13890. - PubMed
-
- de Boer W, Brage S, Kunz R. Insurance medicine in clinical epidemiological terms: A concept paper for discussion. Dutch J Occup Insurance Med (Tijdschrift voor Bedrijfs- en Verzekeringsgeneeskunde - TBV) 2018;26(2):97–99. doi: 10.1007/s12498-018-0040-0. - DOI
-
- Spanjer J, Krol B, Brouwer S, Groothoff JW. Sources of variation in work disability assessment. Work. 2010;37(4):405–411. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
