

Tobacco smoking and risk of 36 cardiovascular disease subtypes: fatal and non-fatal outcomes in a large prospective Australian study
- PMID: 31266500
- PMCID: PMC6607519
- DOI: 10.1186/s12916-019-1351-4
Tobacco smoking and risk of 36 cardiovascular disease subtypes: fatal and non-fatal outcomes in a large prospective Australian study
Abstract
Background: Tobacco smoking is a leading cause of cardiovascular disease (CVD) morbidity and mortality. Evidence on the relation of smoking to different subtypes of CVD, across fatal and non-fatal outcomes, is limited.
Methods: A prospective study of 188,167 CVD- and cancer-free individuals aged ≥ 45 years from the Australian general population joining the 45 and Up Study from 2006 to 2009, with linked questionnaire, hospitalisation and death data up to the end of 2015. Hazard ratios (HRs) for hospitalisation with or mortality from CVD among current and past versus never smokers were estimated, including according to intensity and recency of smoking, using Cox regression, adjusting for age, sex, urban/rural residence, alcohol consumption, income and education. Population-attributable fractions were estimated.
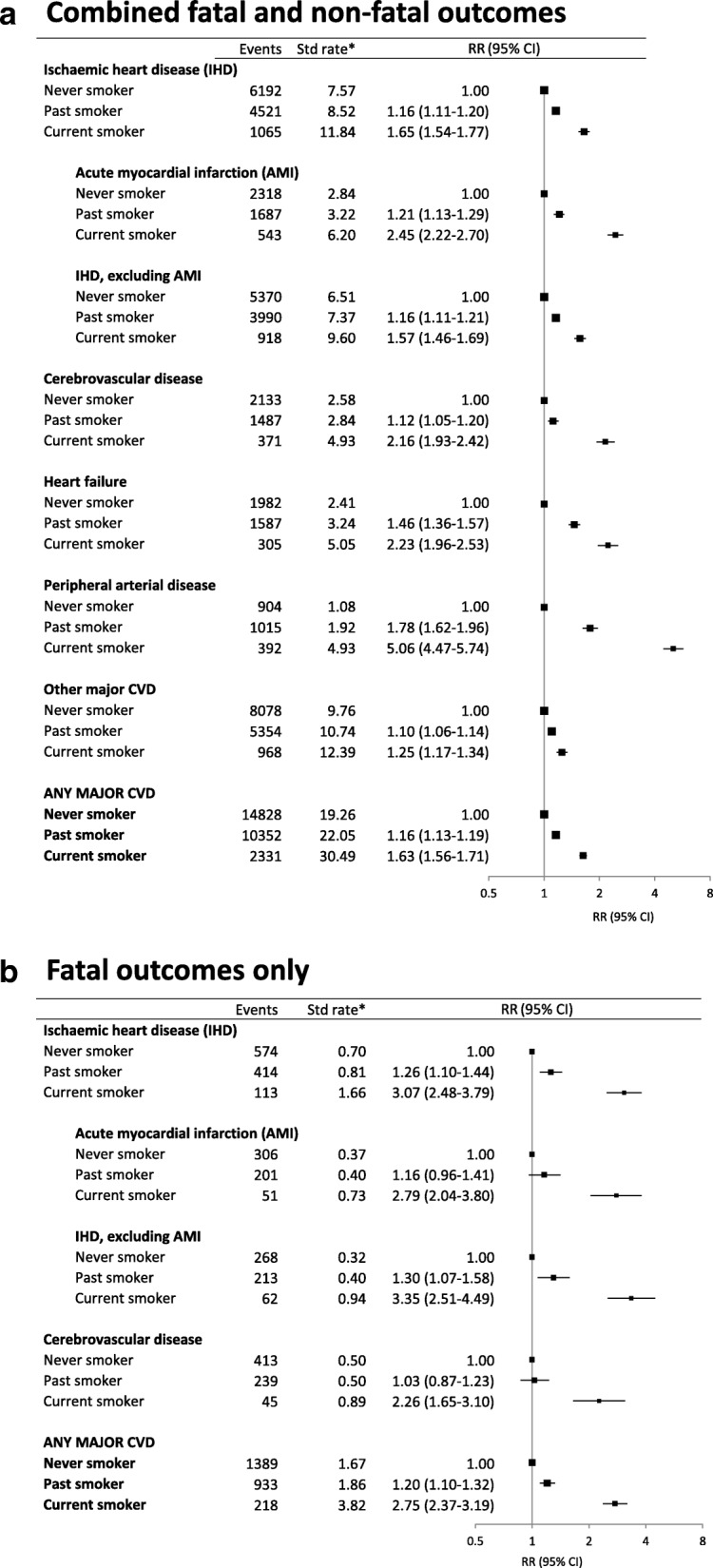
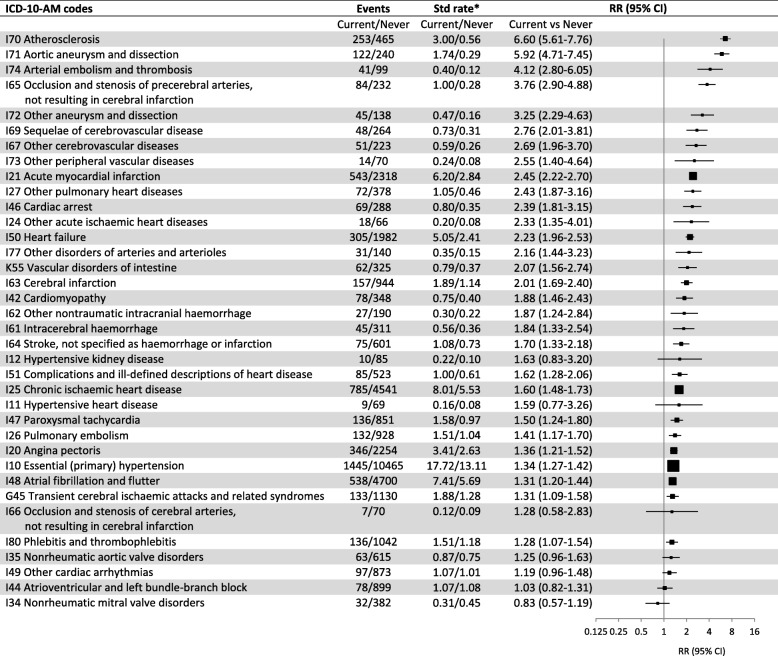
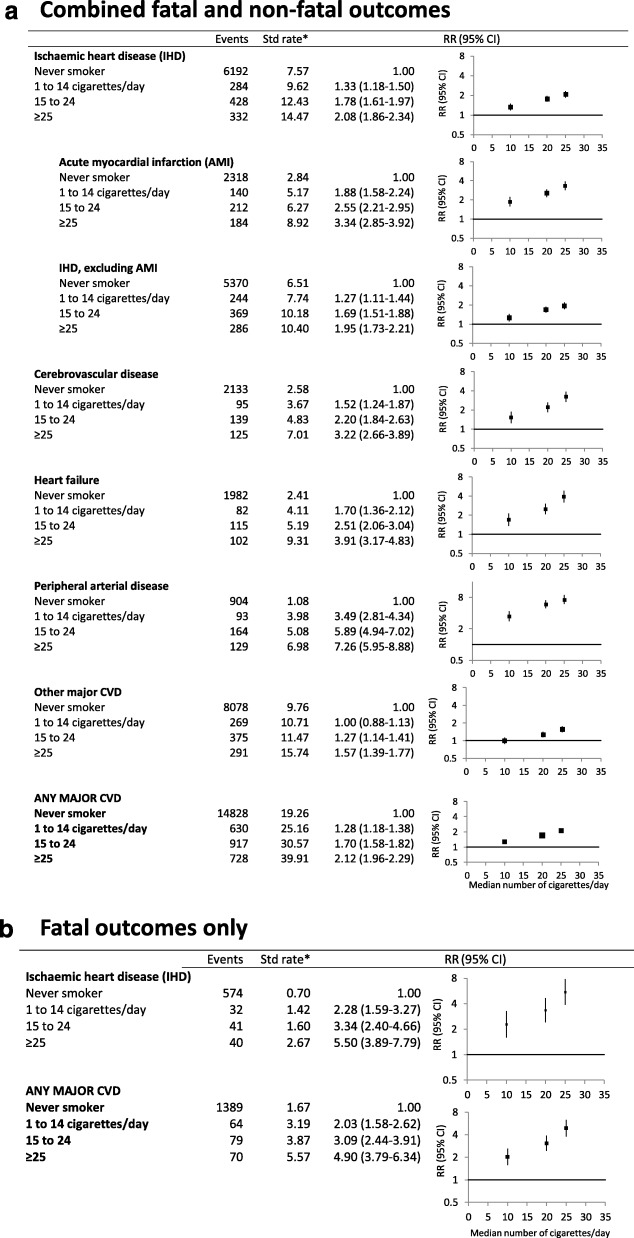
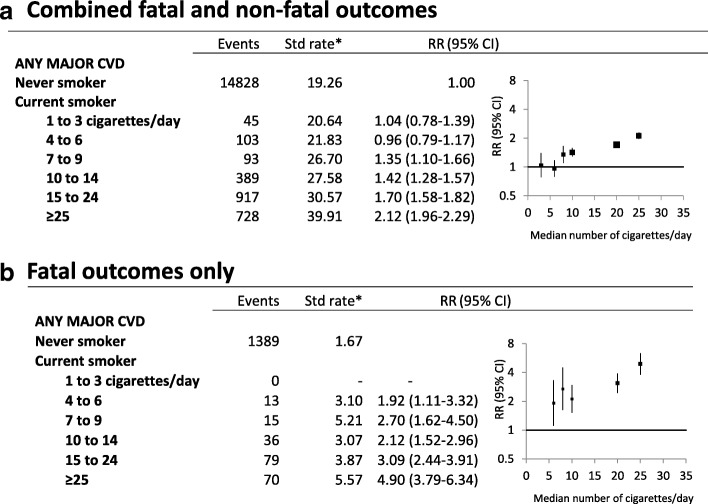
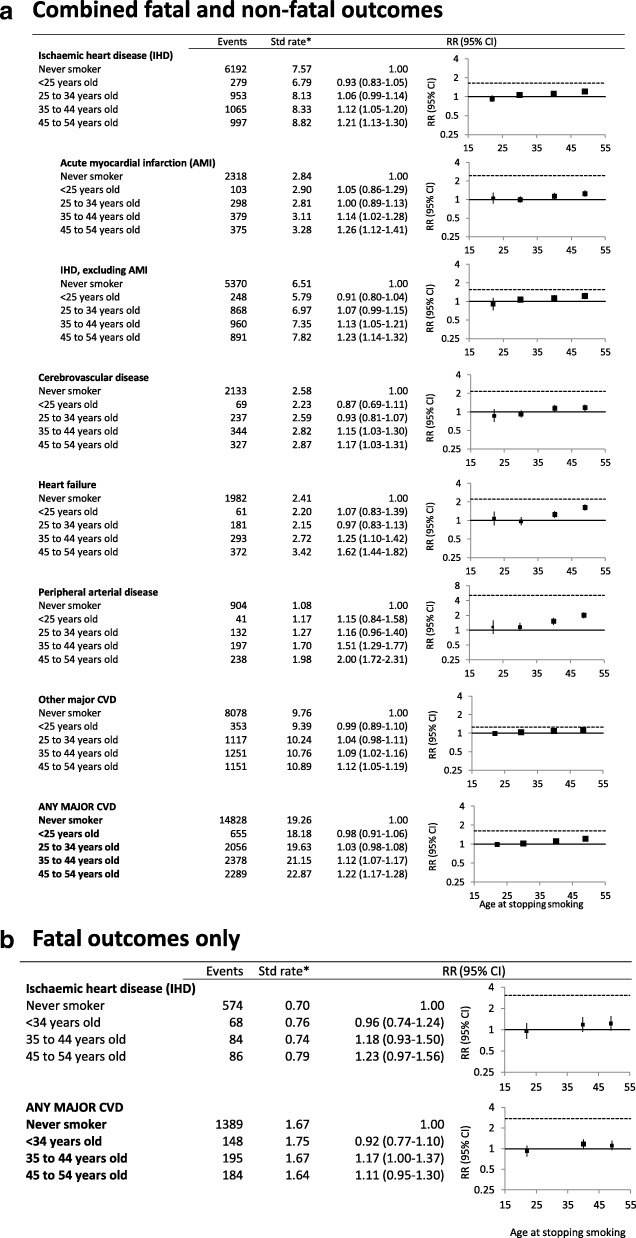
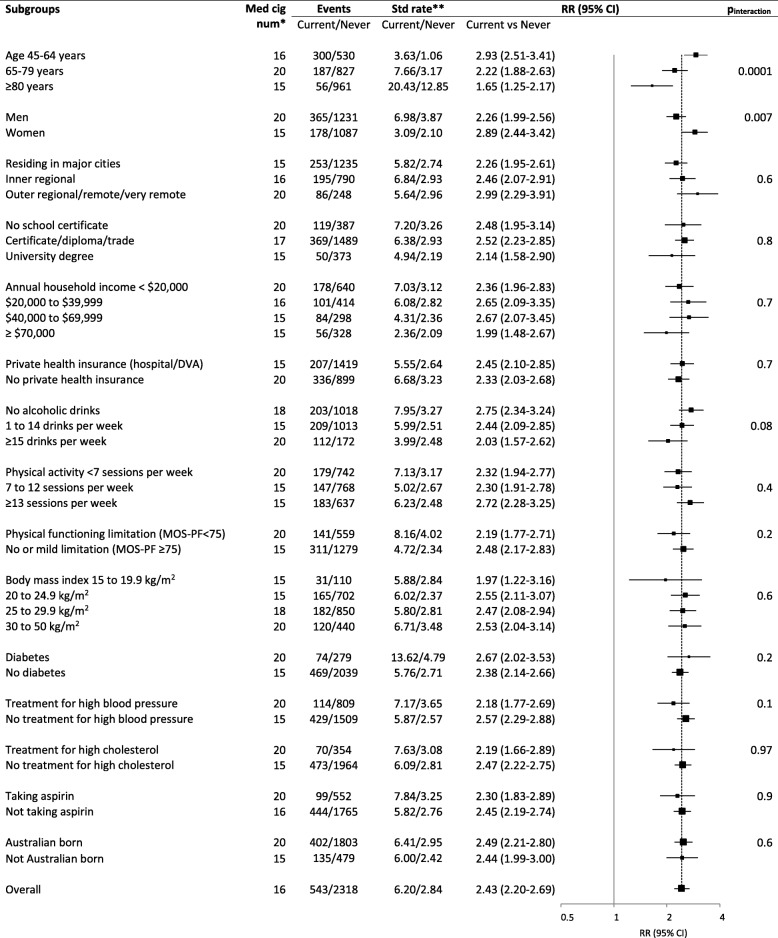
Results: During a mean 7.2 years follow-up (1.35 million person-years), 27,511 (crude rate 20.4/1000 person-years) incident fatal and non-fatal major CVD events occurred, including 4548 (3.2) acute myocardial infarction (AMI), 3991 (2.8) cerebrovascular disease, 3874 (2.7) heart failure and 2311 (1.6) peripheral arterial disease (PAD) events. At baseline, 8% of participants were current and 34% were past smokers. Of the 36 most common specific CVD subtypes, event rates for 29 were increased significantly in current smokers. Adjusted HRs in current versus never smokers were as follows: 1.63 (95%CI 1.56-1.71) for any major CVD, 2.45 (2.22-2.70) for AMI, 2.16 (1.93-2.42) for cerebrovascular disease, 2.23 (1.96-2.53) for heart failure, 5.06 (4.47-5.74) for PAD, 1.50 (1.24-1.80) for paroxysmal tachycardia, 1.31 (1.20-1.44) for atrial fibrillation/flutter, 1.41 (1.17-1.70) for pulmonary embolism, 2.79 (2.04-3.80) for AMI mortality, 2.26 (1.65-3.10) for cerebrovascular disease mortality and 2.75 (2.37-3.19) for total CVD mortality. CVD risks were elevated at almost all levels of current smoking intensity examined and increased with smoking intensity, with HRs for total CVD mortality in current versus never smokers of 1.92 (1.11-3.32) and 4.90 (3.79-6.34) for 4-6 and ≥ 25 cigarettes/day, respectively. Risks diminished with quitting, with excess risks largely avoided by quitting before age 45. Over one third of CVD deaths and one quarter of acute coronary syndrome hospitalisations in Australia aged < 65 can be attributed to smoking.
Conclusions: Current smoking increases the risk of virtually all CVD subtypes, at least doubling the risk of many, including AMI, cerebrovascular disease and heart failure. Paroxysmal tachycardia is a newly identified smoking-related risk. Where comparisons are possible, smoking-associated relative risks for fatal and non-fatal outcomes are similar. Quitting reduces the risk substantially. In an established smoking epidemic, with declining and low current smoking prevalence, smoking accounts for a substantial proportion of premature CVD events.
Keywords: Arrhythmia; Atrial fibrillation; Cardiovascular disease; Cardiovascular mortality; Cerebrovascular disease; Coronary heart disease; Heart failure; Ischaemic heart disease; Smoking; Tobacco.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- GBD 2016 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345–1422. doi: 10.1016/S0140-6736(17)32366-8. - DOI - PMC - PubMed
-
- Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328:1519. doi: 10.1136/bmj.38142.554479.AE. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
