

Analgesic efficacy of preemptive local wound infiltration plus laparoscopic-assisted transversus abdominis plane block versus wound infiltration in patients undergoing laparoscopic colorectal resection: study protocol for a randomized, multicenter, single-blind, noninferiority trial
- PMID: 31266529
- PMCID: PMC6604482
- DOI: 10.1186/s13063-019-3509-y
Analgesic efficacy of preemptive local wound infiltration plus laparoscopic-assisted transversus abdominis plane block versus wound infiltration in patients undergoing laparoscopic colorectal resection: study protocol for a randomized, multicenter, single-blind, noninferiority trial
Abstract
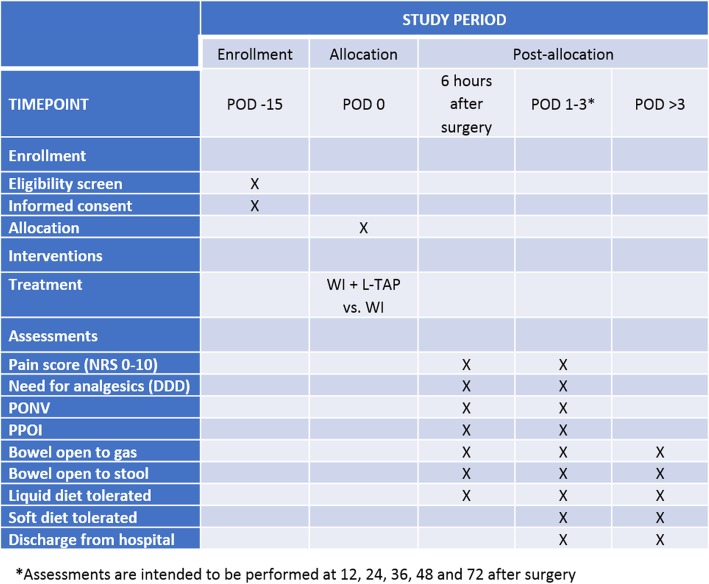
Background: Transversus abdominis plane (TAP) block and wound infiltration (WI) are common locoregional anesthesia techniques for pain management in patients undergoing colorectal laparoscopic surgery. Comparative data between these two practices are conflicting, and a clear benefit of TAP block over WI is still debated. The main purpose of this study is to determine the efficacy in pain control of WI compared with WI plus laparoscopic TAP block (L-TAP) in cases of laparoscopic colorectal resection. Secondary aims are to evaluate other short-term results directly related to pain management: the need for rescue analgesic drugs, the incidence of postoperative nausea and vomiting, the resumption of gut functions, and the length of hospital stay.
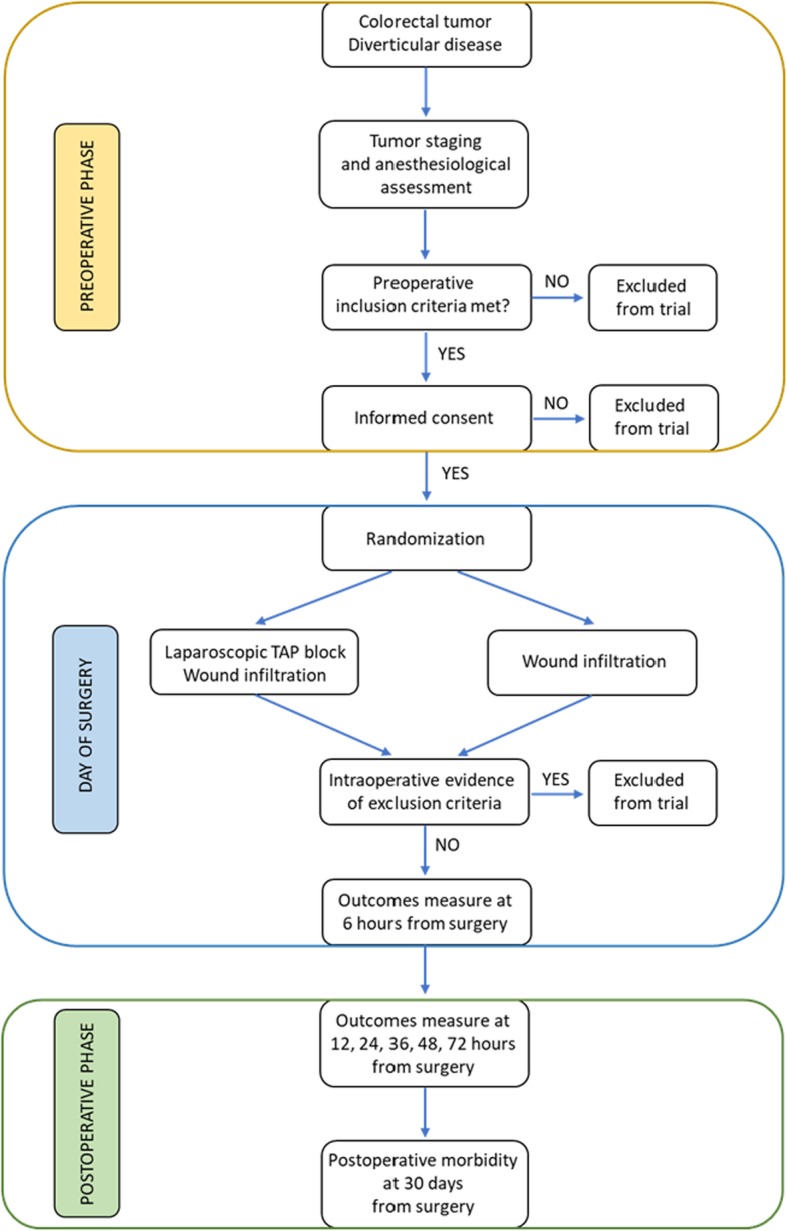
Methods/design: This is a prospective, randomized, controlled, two-arm, multicenter, single-blind study evaluating the efficacy of postoperative analgesic management of WI versus WI plus L-TAP in the context of laparoscopic colorectal surgery. Randomization is at the patient level, and participants are randomized 1:1 to receive either WI alone or WI plus L-TAP. Those eligible for inclusion were patients undergoing laparoscopic resection for colorectal tumor or diverticular disease at the Division of General and Hepatobiliary Surgery, Verona University, Verona, Italy, and at the Colorectal Cancer Center, Kyungpook National University, Daegu, Korea. Fifty-four patients are needed in each group to evidence a difference greater than 1 of 10 according to the numeric rating scale for pain assessment to establish that this difference would matter in practice.
Discussion: The demonstration of a noninferiority of WI compared with WI plus L-TAP block would call into question TAP block usefulness in the setting of laparoscopic colorectal surgery.
Trial registration: ClinicalTrials.gov, NCT03376048 . Prospectively registered on 15 December 2017.
Keywords: Colorectal surgery; Laparoscopy; Postoperative analgesia; TAP block; Wound infiltration.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Analgesic efficacy of pre-emptive local wound infiltration plus laparoscopic-assisted transversus abdominis plane block versus wound infiltration in patients undergoing laparoscopic colorectal resection: results from a randomized, multicenter, single-blind, non-inferiority trial.Surg Endosc. 2021 Jul;35(7):3329-3338. doi: 10.1007/s00464-020-07771-6. Epub 2020 Jul 6. Surg Endosc. 2021. PMID: 32632489 Clinical Trial.
-
Transversus abdominis plane block versus perioperative intravenous lidocaine versus patient-controlled intravenous morphine for postoperative pain control after laparoscopic colorectal surgery: study protocol for a prospective, randomized, double-blind controlled clinical trial.Trials. 2014 Dec 4;15:476. doi: 10.1186/1745-6215-15-476. Trials. 2014. PMID: 25472808 Free PMC article. Clinical Trial.
-
Transversus abdominis plane block for postoperative pain relief after hand-assisted laparoscopic colon surgery: a randomized, placebo-controlled clinical trial.Tech Coloproctol. 2016 Dec;20(12):835-844. doi: 10.1007/s10151-016-1550-3. Epub 2016 Nov 28. Tech Coloproctol. 2016. PMID: 27896461 Clinical Trial.
-
Transversus abdominis plane block using a short-acting local anesthetic for postoperative pain after laparoscopic colorectal surgery: a systematic review and meta-analysis.Surg Endosc. 2018 Feb;32(2):545-552. doi: 10.1007/s00464-017-5871-8. Epub 2017 Oct 26. Surg Endosc. 2018. PMID: 29075970
-
Transversus Abdominis Plane Block versus Wound Infiltration with Conventional Local Anesthetics in Adult Patients Underwent Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials.Biomed Res Int. 2020 Mar 23;2020:8914953. doi: 10.1155/2020/8914953. eCollection 2020. Biomed Res Int. 2020. PMID: 32280705 Free PMC article.
Cited by
-
Transversus Abdominis Plane Block vs. Wound Infiltration for the Reduction of Postoperative Patient-Controlled Analgesia Requirements Following Laparoscopic Hemicolectomy: A Retrospective Case-Control Study.Cureus. 2025 Apr 4;17(4):e81707. doi: 10.7759/cureus.81707. eCollection 2025 Apr. Cureus. 2025. PMID: 40322418 Free PMC article.
-
Updates on Wound Infiltration Use for Postoperative Pain Management: A Narrative Review.J Clin Med. 2021 Oct 11;10(20):4659. doi: 10.3390/jcm10204659. J Clin Med. 2021. PMID: 34682777 Free PMC article. Review.
-
Postoperative Multimodal Analgesia Strategy for Enhanced Recovery After Surgery in Elderly Colorectal Cancer Patients.Pain Ther. 2024 Aug;13(4):745-766. doi: 10.1007/s40122-024-00619-0. Epub 2024 Jun 5. Pain Ther. 2024. PMID: 38836984 Free PMC article. Review.
References
-
- McEvoy MD, Scott MJ, Gordon DB, Grant SA, Thacker JKM, Wu CL, Gan TJ, Mythen MG, Shaw AD, Miller TE, Perioperative Quality Initiative (POQI) Workgroup American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on optimal analgesia within an enhanced recovery pathway for colorectal surgery: part 1—from the preoperative period to PACU. Perioper Med (Lond) 2017;6:8. doi: 10.1186/s13741-017-0064-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
