

WHO Guidelines for Prevention, Care and Treatment of Individuals Infected with HBV: A US Perspective
- PMID: 31266617
- PMCID: PMC9616205
- DOI: 10.1016/j.cld.2019.04.008
WHO Guidelines for Prevention, Care and Treatment of Individuals Infected with HBV: A US Perspective
Abstract
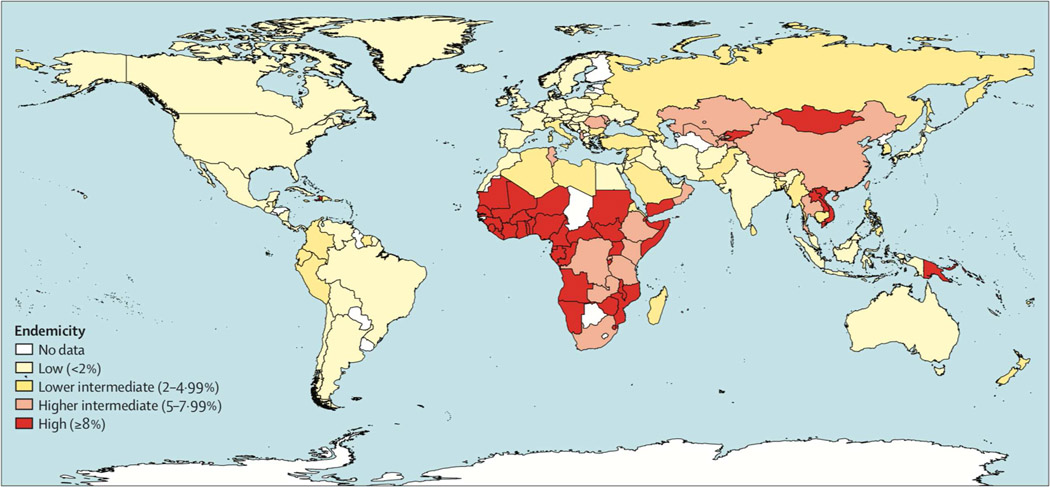
The prevalence of chronic hepatitis B (CHB) differs globally. CHB is responsible for 30% of all deaths from cirrhosis and 40% from hepatocellular carcinoma. The WHO developed guidelines in 2015 on prevention, care, and treatment of chronic HBV infection targeted to program managers in all health care settings, particularly in low- and middle-income countries. Several of the recommendations differ from those of the major Liver Societies, including the American Association for the Study of Liver Diseases (AASLD). This review highlights key differences between the AASLD and WHO guidelines and discusses the impact on management of CHB.
Keywords: AASLD guidelines; Chronic hepatitis B virus Infection; WHO guidelines.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJJTL. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. 2015;386(10003):1546–55. - PubMed
-
- Ott J, Stevens G, Groeger J, Wiersma SJV. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. 2012;30(12):2212–9. - PubMed
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. 2018;392(10159):1789–858. - PMC - PubMed
-
- Organization WH. Global health sector strategy on viral hepatitis 2016–2021. Towards ending viral hepatitis. World Health Organization; 2016.
-
- Organization WH. Guidelines for the Prevention Care and Treatment of Persons with Chronic Hepatitis B Infection: Mar-15: World Health Organization; 2015. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
