

Appendiceal mucinous neoplasm with myxoglobulosis occurring 3 years after perforated barium appendicitis: a case report
- PMID: 31267369
- PMCID: PMC6606682
- DOI: 10.1186/s40792-019-0665-y
Appendiceal mucinous neoplasm with myxoglobulosis occurring 3 years after perforated barium appendicitis: a case report
Abstract
Background: Myxoglobulosis is considered a subtype of appendiceal mucinous neoplasm (AMN). Factors affecting the occurrence of myxoglobulosis include proximal appendiceal obstruction and mucosal secretion at the residual appendiceal mucosa. In addition, myxoglobulosis has also been reportedly associated with persistent chronic inflammation. We report a case of AMN with myxoglobulosis occurring 3 years after perforated barium appendicitis and the importance of caution during surgery for barium peritonitis and elucidate the pathology of myxoglobulosis.
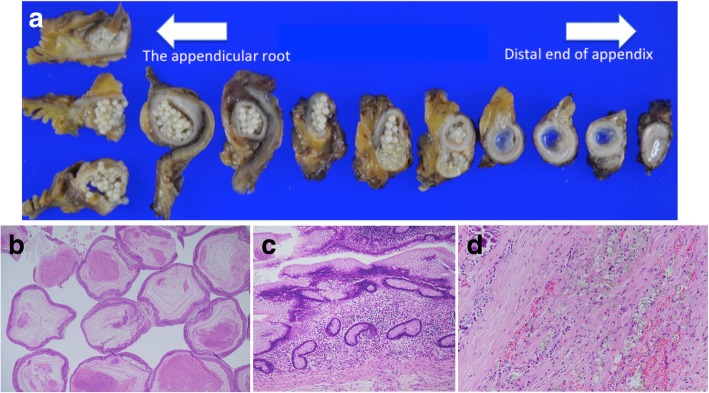
Case presentation: A 45-year-old man with an AMN underwent laparoscopic ileocecal resection 3 years after peritonitis caused by perforated barium appendicitis. The patient had a medical history of perforated barium appendicitis after barium swallow imaging, which was treated conservatively 3 years ago. Computed tomography (CT) revealed cystic enlargement of the appendix and remnant barium around the appendix. He was then pathologically diagnosed with a low-grade AMN based on the resected specimen, and the appendix filled with white globules was diagnosed as myxoglobulosis. When barium is not absorbed, it causes chronic inflammation. As barium was observed around the appendix, prolonged inflammation, and appendicitis may have contributed to the myxoglobulosis. The circumference of the appendix firmly adhered to the surrounding tissue with barium; hence, it was difficult to perform appendectomy. Barium that enters the anastomotic site causes stenosis of this part; therefore, excision of the ileocecal region in the intestinal part where barium is not present was selected instead of appendectomy. Colonoscopy performed 1 year after surgery and showed no evidence of anastomotic stricture.
Conclusion: This case suggested that barium peritonitis caused strong adhesions with the surrounding tissue; thus, careful manipulation was necessary to avoid perforating the appendix. Appendectomy and partial cecal resection were predicted to be difficult because of adhesion by barium. In addition, the ileocecal resection was selected because we had to choose an anastomotic site without barium. The perforated appendicitis caused stenosis of the appendix orifice, and barium surrounding the appendix caused persistent chronic inflammation. This was suggested to contribute to the myxoglobulosis.
Keywords: Appendiceal mucinous neoplasm; Barium appendicitis; Laparoscopic ileocecal resection; Myxoglobulosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Appendiceal neoplasms derived from appendiceal tip remnants following appendectomy: a report of two cases.Surg Case Rep. 2024 Jun 13;10(1):144. doi: 10.1186/s40792-024-01936-4. Surg Case Rep. 2024. PMID: 38867137 Free PMC article.
-
Myxoglobulosis of the appendix.Am J Surg Pathol. 1988 Dec;12(12):962-6. doi: 10.1097/00000478-198812000-00008. Am J Surg Pathol. 1988. PMID: 3202250
-
Emergency laparoscopic ileocecal resection for a low-grade appendiceal mucinous neoplasm with impending rupture: A case report.Int J Surg Case Rep. 2021 Mar;80:105636. doi: 10.1016/j.ijscr.2021.02.022. Epub 2021 Feb 9. Int J Surg Case Rep. 2021. PMID: 33609942 Free PMC article.
-
Appendiceal mucinous cystadenoma presenting as "porcelain" appendix with myxoglobulosis--a rare cause of a right lower quadrant mass.Singapore Med J. 1998 Apr;39(4):174-6. Singapore Med J. 1998. PMID: 9676150 Review.
-
Actinomycosis of the appendix mimicking appendiceal tumor: a case report.World J Gastroenterol. 2010 Jan 21;16(3):395-7. doi: 10.3748/wjg.v16.i3.395. World J Gastroenterol. 2010. PMID: 20082489 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
