

Prognosis of microsatellite instability and/or mismatch repair deficiency stage III colon cancer patients after disease recurrence following adjuvant treatment: results of an ACCENT pooled analysis of seven studies
- PMID: 31268130
- PMCID: PMC7360150
- DOI: 10.1093/annonc/mdz208
Prognosis of microsatellite instability and/or mismatch repair deficiency stage III colon cancer patients after disease recurrence following adjuvant treatment: results of an ACCENT pooled analysis of seven studies
Abstract
Background: Microsatellite instable/deficient mismatch repair (MSI/dMMR) metastatic colorectal cancers have been reported to have a poor prognosis. Frequent co-occurrence of MSI/dMMR and BRAFV600E complicates the association.
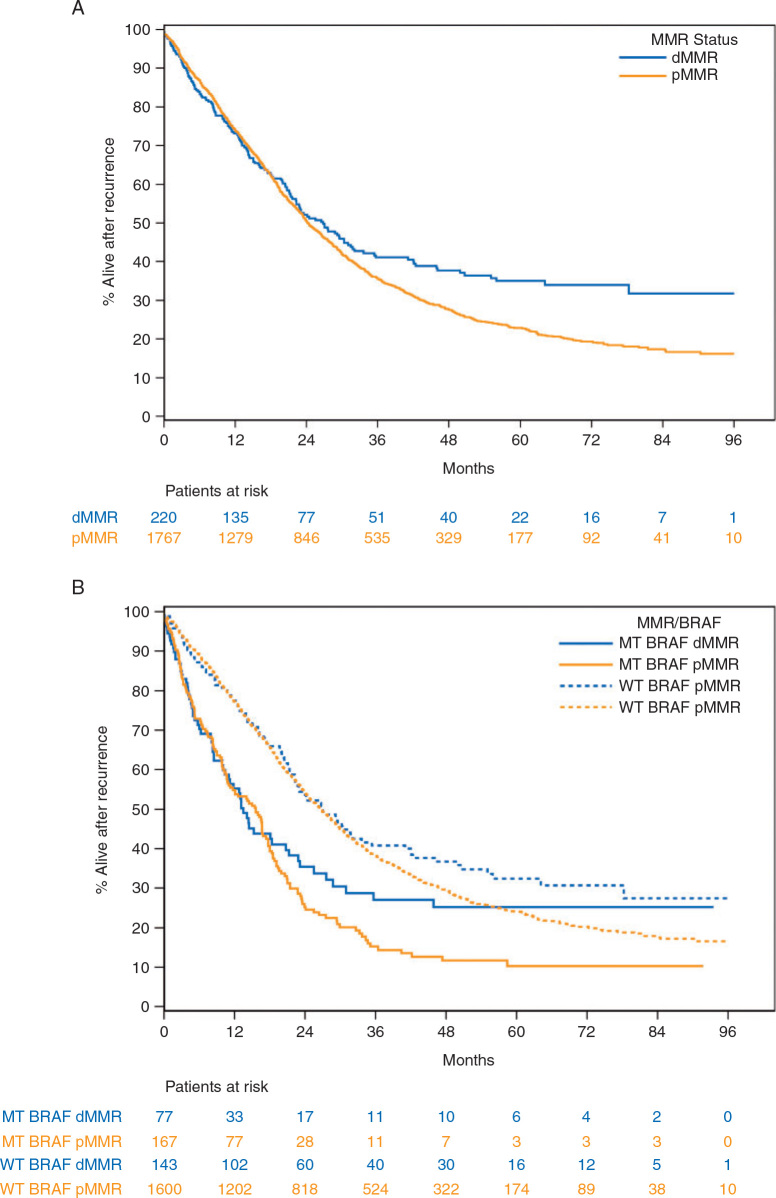
Patients and methods: Patients with resected stage III colon cancer (CC) from seven adjuvant studies with available data for disease recurrence and MMR and BRAFV600E status were analyzed. The primary end point was survival after recurrence (SAR). Associations of markers with SAR were analyzed using Cox proportional hazards models adjusted for age, gender, performance status, T stage, N stage, primary tumor location, grade, KRAS status, and timing of recurrence.
Results: Among 2630 patients with cancer recurrence (1491 men [56.7%], mean age, 58.5 [19-85] years), multivariable analysis revealed that patients with MSI/dMMR tumors had significantly longer SAR than did patients with microsatellite stable/proficient MMR tumors (MSS/pMMR) (adjusted hazard ratio [aHR], 0.82; 95% CI [confidence interval], 0.69-0.98; P = 0.029). This finding remained when looking at patients treated with standard oxaliplatin-based adjuvant chemotherapy regimens only (aHR, 0.76; 95% CI, 0.58-1.00; P = 0.048). Same trends for SAR were observed when analyzing MSI/dMMR versus MSS/pMMR tumor subgroups lacking BRAFV600E (aHR, 0.84; P = 0.10) or those harboring BRAFV600E (aHR, 0.88; P = 0.43), without reaching statistical significance. Furthermore, SAR was significantly shorter in tumors with BRAFV600E versus those lacking this mutation (aHR, 2.06; 95% CI, 1.73-2.46; P < 0.0001), even in the subgroup of MSI/dMMR tumors (aHR, 2.65; 95% CI, 1.67-4.21; P < 0.0001). Other factors associated with a shorter SAR were as follows: older age, male gender, T4/N2, proximal primary tumor location, poorly differentiated adenocarcinoma, and early recurrence.
Conclusions: In stage III CC patients recurring after adjuvant chemotherapy, and before the era of immunotherapy, the MSI/dMMR phenotype was associated with a better SAR compared with MSS/pMMR. BRAFV600E mutation was a poor prognostic factor for both MSI/dMMR and MSS/pMMR patients.
Trial identification numbers: NCT00079274, NCT00265811, NCT00004931, NCT00004931, NCT00026273, NCT00096278, NCT00112918.
Keywords: colon cancer; deficient mismatch repair; microsatellite instability; prognosis; recurrence.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures

Comment in
-
Understanding the clinical behavior of relapsed colon cancers with microsatellite instability relative to BRAF mutations.Ann Oncol. 2019 Sep 1;30(9):1409-1410. doi: 10.1093/annonc/mdz229. Ann Oncol. 2019. PMID: 31350557 No abstract available.
Similar articles
-
Association of DNA Mismatch Repair and Mutations in BRAF and KRAS With Survival After Recurrence in Stage III Colon Cancers : A Secondary Analysis of 2 Randomized Clinical Trials.JAMA Oncol. 2017 Apr 1;3(4):472-480. doi: 10.1001/jamaoncol.2016.5469. JAMA Oncol. 2017. PMID: 28006055 Free PMC article. Clinical Trial.
-
DNA mismatch repair status and colon cancer recurrence and survival in clinical trials of 5-fluorouracil-based adjuvant therapy.J Natl Cancer Inst. 2011 Jun 8;103(11):863-75. doi: 10.1093/jnci/djr153. Epub 2011 May 19. J Natl Cancer Inst. 2011. PMID: 21597022 Free PMC article.
-
Prognostic Value of BRAF and KRAS Mutations in MSI and MSS Stage III Colon Cancer.J Natl Cancer Inst. 2016 Dec 31;109(5):djw272. doi: 10.1093/jnci/djw272. Print 2017 May. J Natl Cancer Inst. 2016. PMID: 28040692 Free PMC article. Clinical Trial.
-
Adjuvant Chemotherapy for Gastric Cancer Patients with Mismatch Repair Deficiency or Microsatellite Instability: Systematic Review and Meta-Analysis.Ann Surg Oncol. 2022 Apr;29(4):2324-2331. doi: 10.1245/s10434-021-11050-6. Epub 2021 Nov 18. Ann Surg Oncol. 2022. PMID: 34796431
-
Microsatellite instability testing and its role in the management of colorectal cancer.Curr Treat Options Oncol. 2015 Jul;16(7):30. doi: 10.1007/s11864-015-0348-2. Curr Treat Options Oncol. 2015. PMID: 26031544 Free PMC article. Review.
Cited by
-
Comprehensive Review of Biomarkers for the Treatment of Locally Advanced Colon Cancer.Cells. 2022 Nov 23;11(23):3744. doi: 10.3390/cells11233744. Cells. 2022. PMID: 36497002 Free PMC article. Review.
-
A Truncated NRIP1 Mutant Amplifies Microsatellite Instability of Colorectal Cancer by Regulating MSH2/MSH6 Expression, and Is a Prognostic Marker of Stage III Tumors.Cancers (Basel). 2021 Sep 3;13(17):4449. doi: 10.3390/cancers13174449. Cancers (Basel). 2021. PMID: 34503257 Free PMC article.
-
What is the significance of mismatch repair deficiency in stage IV colon cancer?J Gastrointest Oncol. 2025 Feb 28;16(1):330-332. doi: 10.21037/jgo-2025-74. Epub 2025 Feb 25. J Gastrointest Oncol. 2025. PMID: 40115933 Free PMC article. No abstract available.
-
Neoantigens and their clinical applications in human gastrointestinal cancers.World J Surg Oncol. 2022 Sep 29;20(1):321. doi: 10.1186/s12957-022-02776-y. World J Surg Oncol. 2022. PMID: 36171610 Free PMC article. Review.
-
Colorectal Cancer Immunotherapy: State of the Art and Future Directions.Gastro Hep Adv. 2023;2(8):1103-1119. doi: 10.1016/j.gastha.2023.09.007. Epub 2023 Sep 19. Gastro Hep Adv. 2023. PMID: 38098742 Free PMC article.
References
-
- Taieb J., André T., Auclin E. Refining adjuvant therapy for non-metastatic colon cancer, new standards and perspectives. Cancer Treat Rev. 2019;75:1–11. - PubMed
-
- André T., Boni C., Mounedji-Boudiaf L. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350(23):2343–2351. - PubMed
-
- Van Cutsem E., Labianca R., Bodoky G. Randomized phase III trial comparing biweekly infusional fluorouracil/leucovorin alone or with irinotecan in the adjuvant treatment of stage III colon cancer: pETACC-3. J Clin Oncol. 2009;27(19):3117–3125. - PubMed
-
- de Gramont A., Van Cutsem E., Schmoll H.-J. Bevacizumab plus oxaliplatin-based chemotherapy as adjuvant treatment for colon cancer (AVANT): a phase 3 randomised controlled trial. Lancet Oncol. 2012;13(12):1225–1233. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
