

A Quantitative Severity Scale for Retinopathy of Prematurity Using Deep Learning to Monitor Disease Regression After Treatment
- PMID: 31268499
- PMCID: PMC6613298
- DOI: 10.1001/jamaophthalmol.2019.2442
A Quantitative Severity Scale for Retinopathy of Prematurity Using Deep Learning to Monitor Disease Regression After Treatment
Abstract
Importance: Retinopathy of prematurity (ROP) is a leading cause of childhood blindness worldwide, but treatment failure and disease recurrence are important causes of adverse outcomes in patients with treatment-requiring ROP (TR-ROP).
Objectives: To apply an automated ROP vascular severity score obtained using a deep learning algorithm and to assess its utility for objectively monitoring ROP regression after treatment.
Design, setting, and participants: This retrospective cohort study used data from the Imaging and Informatics in ROP consortium, which comprises 9 tertiary referral centers in North America that screen high volumes of at-risk infants for ROP. Images of 5255 clinical eye examinations from 871 infants performed between July 2011 and December 2016 were assessed for eligibility in the present study. The disease course was assessed with time across the numerous examinations for patients with TR-ROP. Infants born prematurely meeting screening criteria for ROP who developed TR-ROP and who had images captured within 4 weeks before and after treatment as well as at the time of treatment were included.
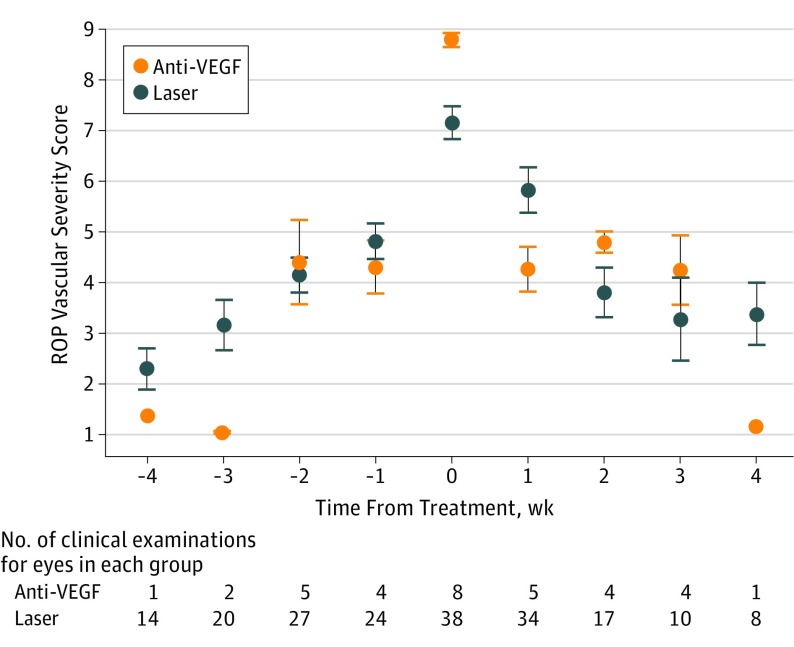
Main outcomes and measures: The primary outcome was mean (SD) ROP vascular severity score before, at time of, and after treatment. A deep learning classifier was used to assign a continuous ROP vascular severity score, which ranged from 1 (normal) to 9 (most severe), at each examination. A secondary outcome was the difference in ROP vascular severity score among eyes treated with laser or the vascular endothelial growth factor antagonist bevacizumab. Differences between groups for both outcomes were assessed using unpaired 2-tailed t tests with Bonferroni correction.
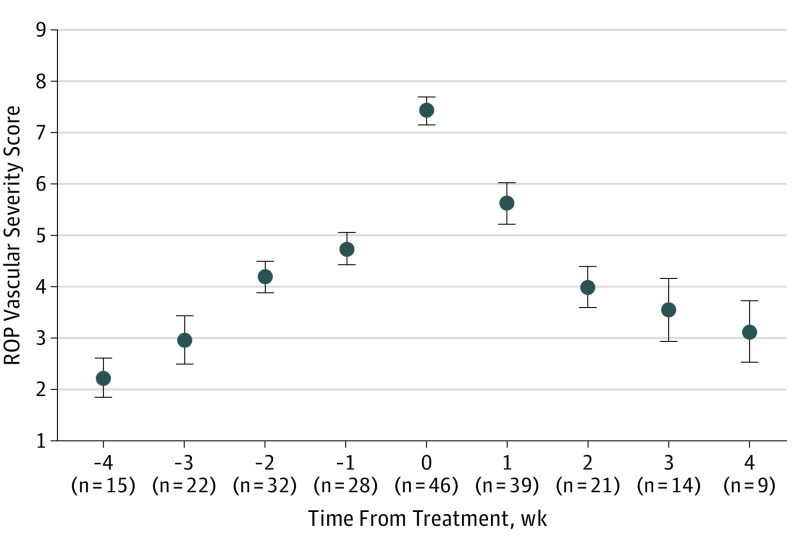
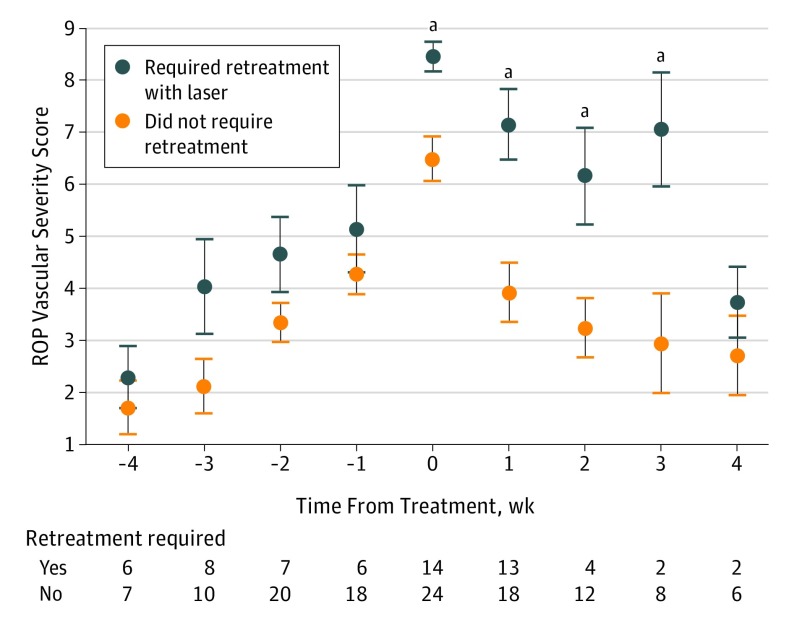
Results: Of 5255 examined eyes, 91 developed TR-ROP, of which 46 eyes met the inclusion criteria based on the available images. The mean (SD) birth weight of those patients was 653 (185) g, with a mean (SD) gestational age of 24.9 (1.3) weeks. The mean (SD) ROP vascular severity scores significantly increased 2 weeks prior to treatment (4.19 [1.75]), peaked at treatment (7.43 [1.89]), and decreased for at least 2 weeks after treatment (4.00 [1.88]) (all P < .001). Eyes requiring retreatment with laser had higher ROP vascular severity scores at the time of initial treatment compared with eyes receiving a single treatment (P < .001).
Conclusions and relevance: This quantitative ROP vascular severity score appears to consistently reflect clinical disease progression and posttreatment regression in eyes with TR-ROP. These study results may have implications for the monitoring of patients with ROP for treatment failure and disease recurrence and for determining the appropriate level of disease severity for primary treatment in eyes with aggressive disease.
Conflict of interest statement
Figures


Comment on
-
Automated Algorithms and Retinopathy of Prematurity Treatment.JAMA Ophthalmol. 2019 Sep 1;137(9):1036-1037. doi: 10.1001/jamaophthalmol.2019.2463. JAMA Ophthalmol. 2019. PMID: 31268515 No abstract available.
References
-
- Early Treatment For Retinopathy Of Prematurity Cooperative Group Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol. 2003;121(12):1684-1694. doi:10.1001/archopht.121.12.1684 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
