

Mineral and bone disorder in hemodialysis patients in the Tibetan Plateau: a multicenter cross-sectional study
- PMID: 31269846
- PMCID: PMC6610496
- DOI: 10.1080/0886022X.2019.1635892
Mineral and bone disorder in hemodialysis patients in the Tibetan Plateau: a multicenter cross-sectional study
Erratum in
-
Correction.Ren Fail. 2021 Dec;43(1):878. doi: 10.1080/0886022X.2021.1927335. Ren Fail. 2021. PMID: 34044742 Free PMC article. No abstract available.
Abstract
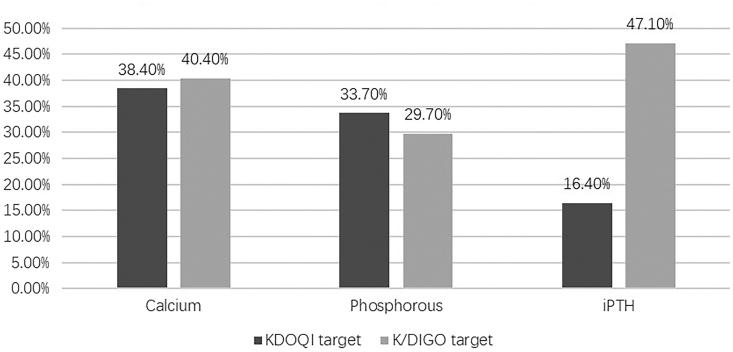
Background: Mineral and bone disorder (MBD) in hemodialysis patients is associated with increased morbidity and mortality. Studies on the MBD status of hemodialysis patients at high altitudes are extremely limited. Methods: A total of 146 hemodialysis patients from 5 local hospitals across all districts with hemodialysis centers in the Tibetan Plateau were enrolled in this cross-sectional study. Parameters related to MBD, including serum phosphorus (P), calcium (Ca), and intact parathyroid hormone (iPTH) levels, were measured. The achievement of MBD goals was compared with the achievement in the Dialysis Outcomes and Practice Study (DOPPS) 3, DOPPS 4 and a multicenter study of MBD in China. Factors associated with hyperphosphatemia were examined. Results: Altogether, 146 hemodialysis patients were recruited from the Tibetan Plateau. According to the K/DIGO guidelines, there were low achievement rates for serum Ca (40.4%), P (29.7%), and iPTH (47.1%). As for the (KDOQI) guidelines, the rates of achievement of defined targets were 38.4%, 33.7% and 16.4% for serum Ca, P and iPTH, respectively. The percentages of patients reaching the KDOQI targets for corrected Ca, P, and iPTH were significantly lower for Tibetan patients than the percentages found in DOPPS 3 (38.4% vs. 50.4%, 33.7% vs. 49.8%, and 16.4% vs. 31.4%, respectively, all p < .001) and DOPPS 4 (38.4% vs. 56.0%, 33.7% vs. 54.5%, and 16.4% vs. 35.3%, respectively, all p < .001). The percentage of patients reaching the KDOQI targets for iPTH was significantly lower in Tibet than in the plain areas of China (16.4% vs. 26.5%, p < .001). The proportion of patients with hypocalcemia was higher in Tibet than in the plain areas (44.5% vs. 19.4%, p < .001). The percentage of local patients with optimal P was significantly higher for patients with an activated vitamin D prescription than for patients without an activated vitamin D prescription (45.3% vs. 19.3%, p < .001). Age and the activated vitamin D prescription were independently associated with hyperphosphatemia. Conclusion: The MBD status of hemodialysis patients in Tibet is far from the ideal level. High altitude is one of the possible causes of the differences found, but not the principal one. It is necessary for medical staff in Tibet to improve the detection and treatment of MBD.
Keywords: End stage renal disease; MBD; Tibet; hemodialysis; high altitude.
Figures
References
-
- Moe SM, Drueke T, Lameire N, et al. . Chronic kidney disease-mineral-bone disorder: a new paradigm. Adv Chronic Kidney Dis. 2007;14:3–12. - PubMed
-
- Martin KJ, Gonzalez EA. Prevention and control of phosphate retention/hyperphosphatemia in CKD-MBD: what is normal, when to start, and how to treat? Cjasn. 2011;6:440–446. - PubMed
-
- Tentori F. Mineral and bone disorder and outcomes in hemodialysis patients: results from the DOPPS. Semin Dial. 2010;23:10–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials