

Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) versus low PEEP on patients with moderate-severe acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials
- PMID: 31269867
- PMCID: PMC6611025
- DOI: 10.1177/1753466619858228
Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) versus low PEEP on patients with moderate-severe acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Setting a positive end-expiratory pressure (PEEP) on patients with acute respiratory distress syndrome (ARDS) receiving mechanical ventilation has been an issue of great contention. Therefore, we aimed to determine effects of lung recruitment maneuver (RM) and titrated PEEP versus low PEEP on adult patients with moderate-severe ARDS.
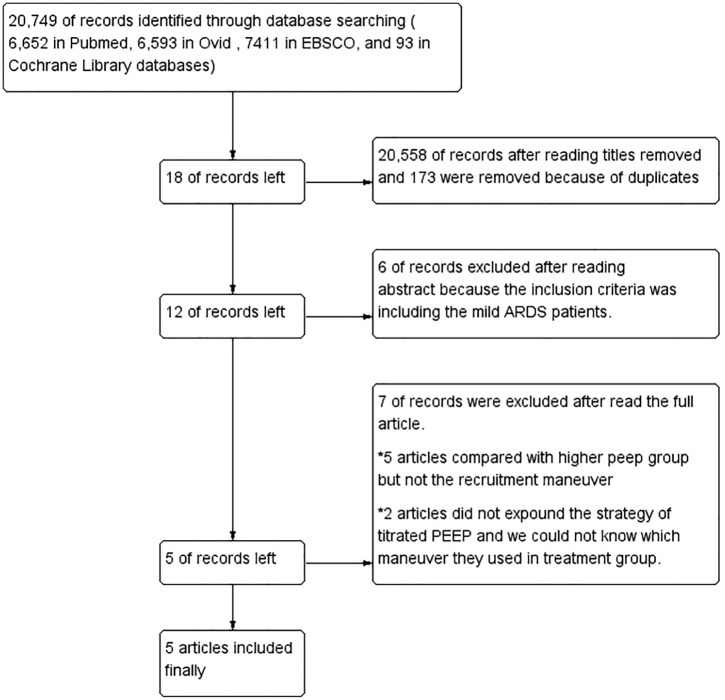
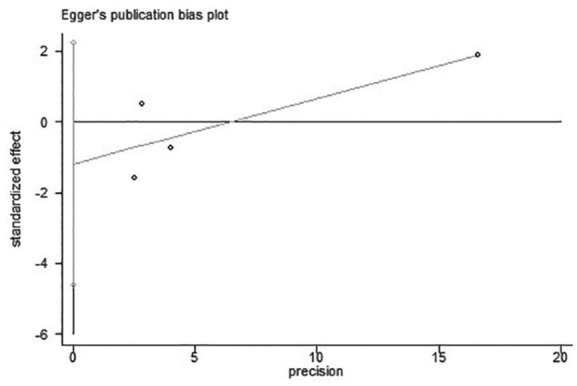
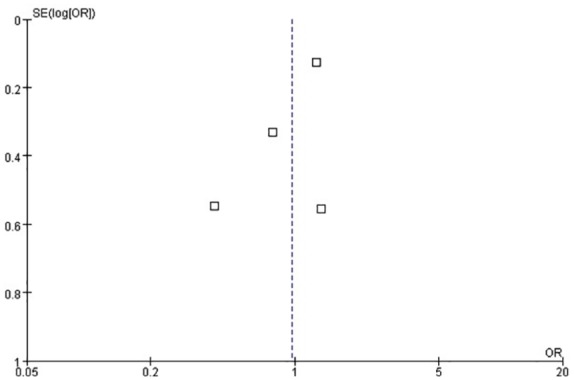
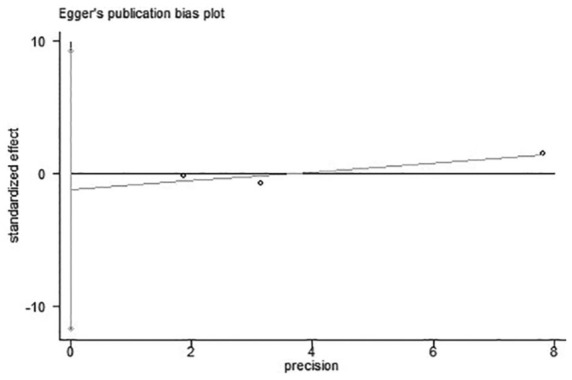
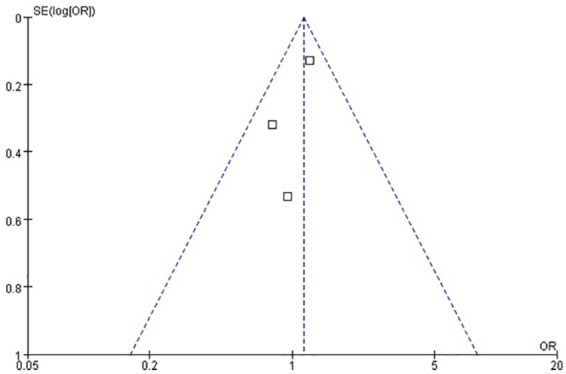
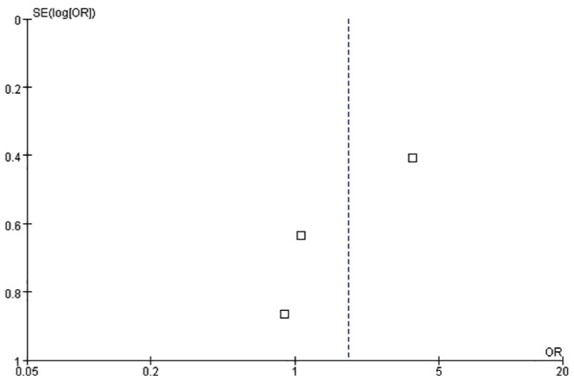
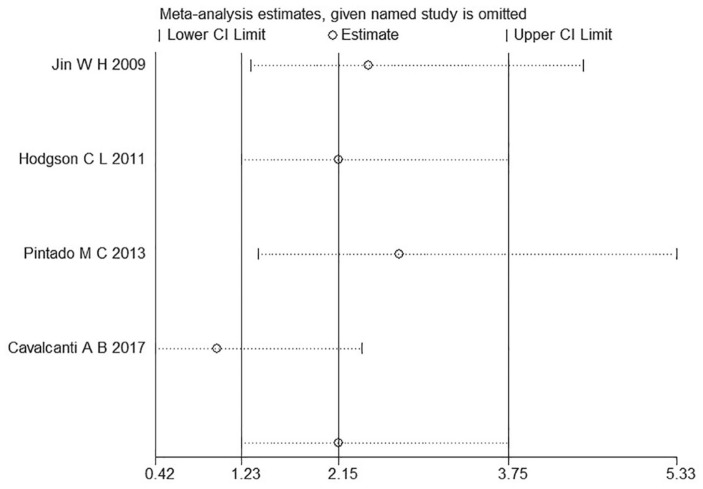
Methods: Data sources and study selection proceeded as follows: PubMed, Ovid, EBSCO, and Cochrane Library databases were searched from 2003 to May 2018. Original clinical randomized controlled trials which met the eligibility criteria were included. To compare the prognosis between the titrated PEEP and low PEEP groups on patients with moderate-severe ARDS (PaO2/FiO2 < 200 mmHg). Heterogeneity was quantified through the I2 statistic. Egger's test and funnel plots were used to assess publication bias.
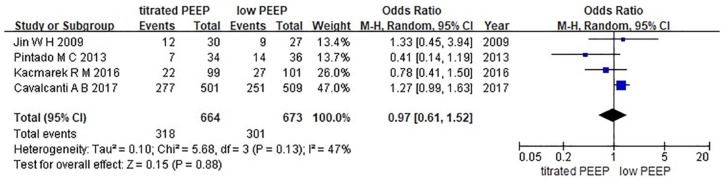
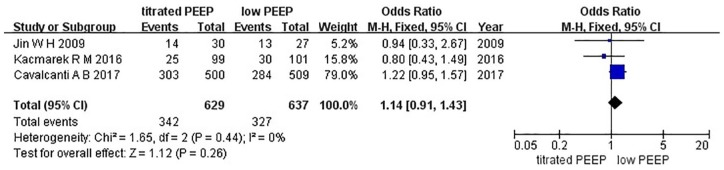
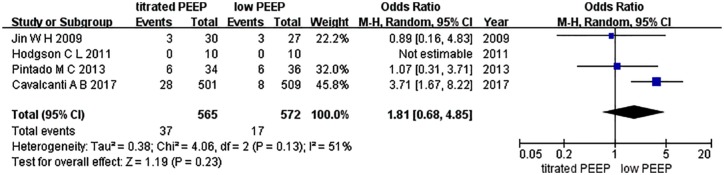
Results: No difference was found in 28-day mortality and ICU mortality (OR = 0.97, 95% CI (0.61-1.52), p = 0.88; OR = 1.14, 95% CI (0.91-1.43), p = 0.26, respectively). Only ventilator-free days, length of stay in the ICU, length of stay in hospital, and incidence of barotrauma could be systematically reviewed owing to bias and extensive heterogeneity.
Conclusion: No difference was observed in the RM between the titrated PEEP and the low PEEP in 28-day mortality and ICU mortality on patients with moderate-severe ARDS.
Keywords: acute respiratory distress syndrome; meta-analysis; mortality; positive end-expiratory pressure; systematic review.
Conflict of interest statement
Figures
Similar articles
-
High versus low positive end-expiratory pressure (PEEP) levels for mechanically ventilated adult patients with acute lung injury and acute respiratory distress syndrome.Cochrane Database Syst Rev. 2021 Mar 30;3(3):CD009098. doi: 10.1002/14651858.CD009098.pub3. Cochrane Database Syst Rev. 2021. PMID: 33784416 Free PMC article.
-
The impact of a lung-protective ventilation mode using transpulmonary driving pressure titrated positive end-expiratory pressure on the prognosis of patients with acute respiratory distress syndrome.J Clin Monit Comput. 2024 Dec;38(6):1405-1414. doi: 10.1007/s10877-024-01198-3. Epub 2024 Aug 19. J Clin Monit Comput. 2024. PMID: 39158781 Clinical Trial.
-
Effect of Lung Recruitment and Titrated Positive End-Expiratory Pressure (PEEP) vs Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial.JAMA. 2017 Oct 10;318(14):1335-1345. doi: 10.1001/jama.2017.14171. JAMA. 2017. PMID: 28973363 Free PMC article. Clinical Trial.
-
Effect of Titrating Positive End-Expiratory Pressure (PEEP) With an Esophageal Pressure-Guided Strategy vs an Empirical High PEEP-Fio2 Strategy on Death and Days Free From Mechanical Ventilation Among Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial.JAMA. 2019 Mar 5;321(9):846-857. doi: 10.1001/jama.2019.0555. JAMA. 2019. PMID: 30776290 Free PMC article. Clinical Trial.
-
Higher PEEP versus lower PEEP strategies for patients in ICU without acute respiratory distress syndrome: A systematic review and meta-analysis.J Crit Care. 2022 Feb;67:72-78. doi: 10.1016/j.jcrc.2021.09.026. Epub 2021 Oct 21. J Crit Care. 2022. PMID: 34689064
Cited by
-
A Physiologically Informed Strategy to Effectively Open, Stabilize, and Protect the Acutely Injured Lung.Front Physiol. 2020 Mar 19;11:227. doi: 10.3389/fphys.2020.00227. eCollection 2020. Front Physiol. 2020. PMID: 32265734 Free PMC article. Review.
-
High versus low positive end-expiratory pressure (PEEP) levels for mechanically ventilated adult patients with acute lung injury and acute respiratory distress syndrome.Cochrane Database Syst Rev. 2021 Mar 30;3(3):CD009098. doi: 10.1002/14651858.CD009098.pub3. Cochrane Database Syst Rev. 2021. PMID: 33784416 Free PMC article.
-
[Estimation of lung recruitment characteristics using the static pressure-volume curve of lungs].Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2021 Apr 25;38(2):326-332. doi: 10.7507/1001-5515.202008061. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2021. PMID: 33913293 Free PMC article. Chinese.
-
Pulmonary Barotrauma Resulting from Mechanical Ventilation in 2 Patients with a Diagnosis of COVID-19 Pneumonia.Am J Case Rep. 2021 Jan 27;22:e927954. doi: 10.12659/AJCR.927954. Am J Case Rep. 2021. PMID: 33500377 Free PMC article.
References
-
- Uzawa T, Ashbaugh DG. Continuous positive-pressure breathing in acute hemorrhagic pulmonary edema. J Appl Physiol 1969; 26: 427–432. - PubMed
-
- Suzumura EA, Amato MB, Cavalcanti AB. Understanding recruitment maneuvers. Intensive Care Med 2016; 42: 908–911. - PubMed
-
- Nieman GF, Gatto LA, Habashi NM. The impact of mechanical ventilation on the pathophysiology of progressive acute lung injury. J Appl Physiol 2015; 119: 1245–1261. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
