

Gender but not diabetes, hypertension or smoking affects infarct evolution in ST-elevation myocardial infarction patients - data from the CHILL-MI, MITOCARE and SOCCER trials
- PMID: 31269907
- PMCID: PMC6610840
- DOI: 10.1186/s12872-019-1139-7
Gender but not diabetes, hypertension or smoking affects infarct evolution in ST-elevation myocardial infarction patients - data from the CHILL-MI, MITOCARE and SOCCER trials
Abstract
Background: Infarct evolution rate and response to acute reperfusion therapy may differ between patients, which is important to consider for accurate management and treatment of patients with ST-elevation myocardial infarction (STEMI). The aim of this study was therefore to investigate the association of infarct size and myocardial salvage with gender, smoking status, presence of diabetes or history of hypertension in a cohort of STEMI-patients.
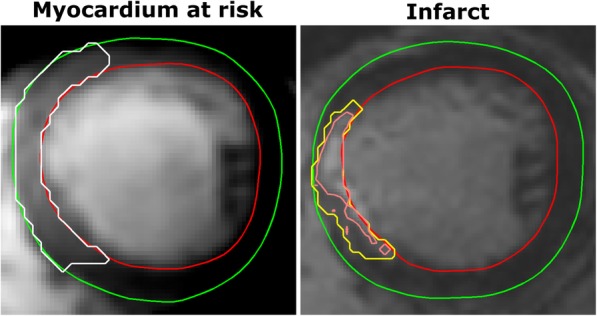
Methods: Patients (n = 301) with first-time STEMI from the three recent multi-center trials (CHILL-MI, MITOCARE and SOCCER) underwent cardiac magnetic resonance (CMR) imaging to determine myocardium at risk (MaR) and infarct size (IS). Myocardial salvage index (MSI) was calculated as MSI = 1-IS/MaR. Pain to balloon time, culprit vessel, trial treatments, age, TIMI grade flow and collateral flow by Rentrop grading were included as explanatory variables in the statistical model.
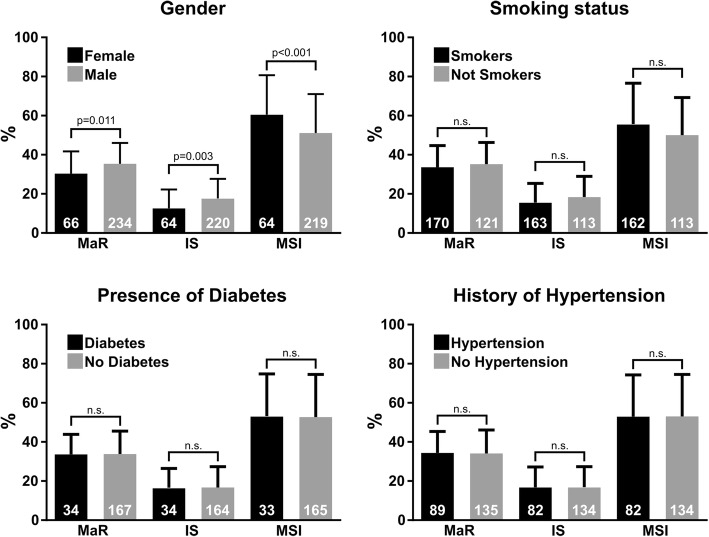
Results: Women (n = 66) had significantly smaller MaR (mean difference: 5.0 ± 1.5% of left ventricle (LV), p < 0.01), smaller IS (mean difference: 5.1 ± 1.4% of LV, p = 0.03), and larger MSI (mean difference: 9.6 ± 2.8% of LV, p < 0.01) compared to men (n = 238). These differences remained significant when adjusting for other explanatory variables. There were no significant effects on MaR, IS or MSI for diabetes, hypertension or smoking.
Conclusions: Female gender is associated with higher myocardial salvage and smaller infarct size suggesting a pathophysiological difference in infarct evolution between men and women.
Keywords: Area at risk; Diabetes; Gender; Hypertension; Sex.
Conflict of interest statement
Dr. Arheden is a shareholder of Imacor. Drs Arheden, Heiberg, Carlsson, and Engblom consult for Imacor, the core-lab that performed the CMR-analysis for the MITOCARE, CHILL-MI, and SOCCER trials. Dr. Heiberg is the founder and owner of the company Medviso AB, Lund, Sweden. The authors declare that they have no competing interests.
Figures
References
-
- Wu E, Ortiz JT, Tejedor P, Lee DC, Bucciarelli-Ducci C, Kansal P, Carr JC, Holly TA, Lloyd-Jones D, Klocke FJ, Bonow RO. Infarct size by contrast enhanced cardiac magnetic resonance is a stronger predictor of outcomes than left ventricular ejection fraction or end-systolic volume index: prospective cohort study. Heart. 2008;94:730–736. doi: 10.1136/hrt.2007.122622. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
