

Prenatal diagnosis and prevalence of critical congenital heart defects: an international retrospective cohort study
- PMID: 31270117
- PMCID: PMC6609145
- DOI: 10.1136/bmjopen-2018-028139
Prenatal diagnosis and prevalence of critical congenital heart defects: an international retrospective cohort study
Abstract
Objectives: To assess international trends and patterns of prenatal diagnosis of critical congenital heart defects (CCHDs) and their relation to total and live birth CCHD prevalence and mortality.
Setting: Fifteen birth defect surveillance programmes that participate in the International Clearinghouse for Birth Defects Surveillance and Research from 12 countries in Europe, North and South America and Asia.
Participants: Live births, stillbirths and elective terminations of pregnancy for fetal anomaly diagnosed with 1 of 12 selected CCHD, ascertained by the 15 programmes for delivery years 2000 to 2014.
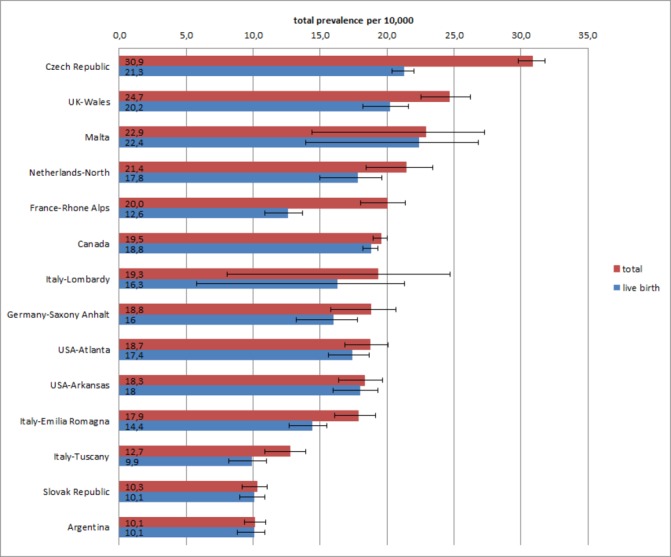
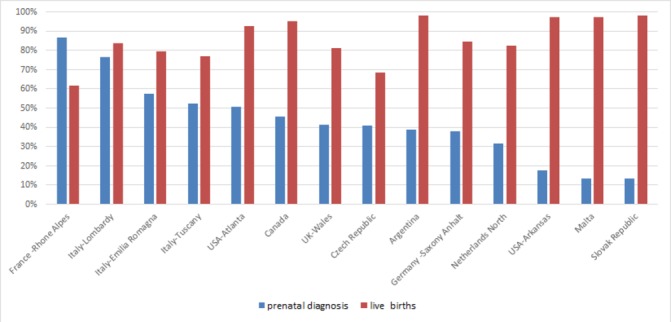
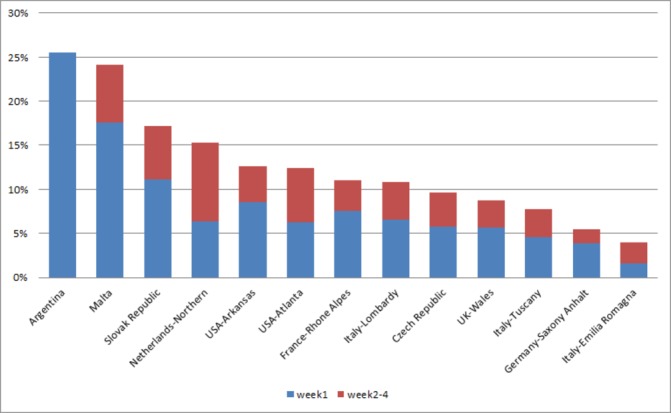
Results: 18 243 CCHD cases were reported among 8 847 081 births. The median total prevalence was 19.1 per 10 000 births but varied threefold between programmes from 10.1 to 31.0 per 10 000. CCHD were prenatally detected for at least 50% of the cases in one-third of the programmes. However, prenatal detection varied from 13% in Slovak Republic to 87% in some areas in France. Prenatal detection was consistently high for hypoplastic left heart syndrome (64% overall) and was lowest for total anomalous pulmonary venous return (28% overall). Surveillance programmes in countries that do not legally permit terminations of pregnancy tended to have higher live birth prevalence of CCHD. Most programmes showed an increasing trend in prenatally diagnosed CCHD cases.
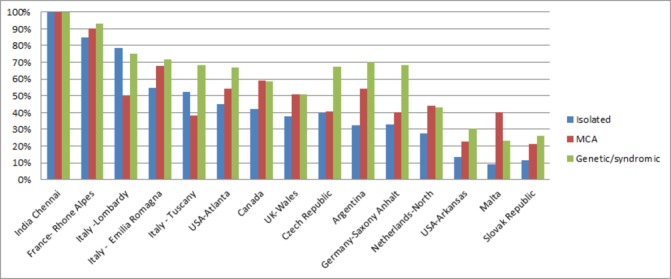
Discussion and conclusions: Prenatal detection already accounts for 50% or more of CCHD detected in many programmes and is increasing. Local policies and access likely account for the wide variability of reported occurrence and prenatal diagnosis. Detection rates are high especially for CCHD that are more easily diagnosed on a standard obstetric four-chamber ultrasound or for fetuses that have extracardiac anomalies. These ongoing trends in prenatal diagnosis, potentially in combination with newborn pulse oximetry, are likely to modify the epidemiology and clinical outcomes of CCHD in the near future.
Keywords: critical congenital heart defects; epidemiology; prenatal diagnosis.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical