

Effects of Iliac Stenosis on Abdominal Aortic Aneurysm Formation in Mice and Humans
- PMID: 31272099
- PMCID: PMC6819217
- DOI: 10.1159/000501312
Effects of Iliac Stenosis on Abdominal Aortic Aneurysm Formation in Mice and Humans
Abstract
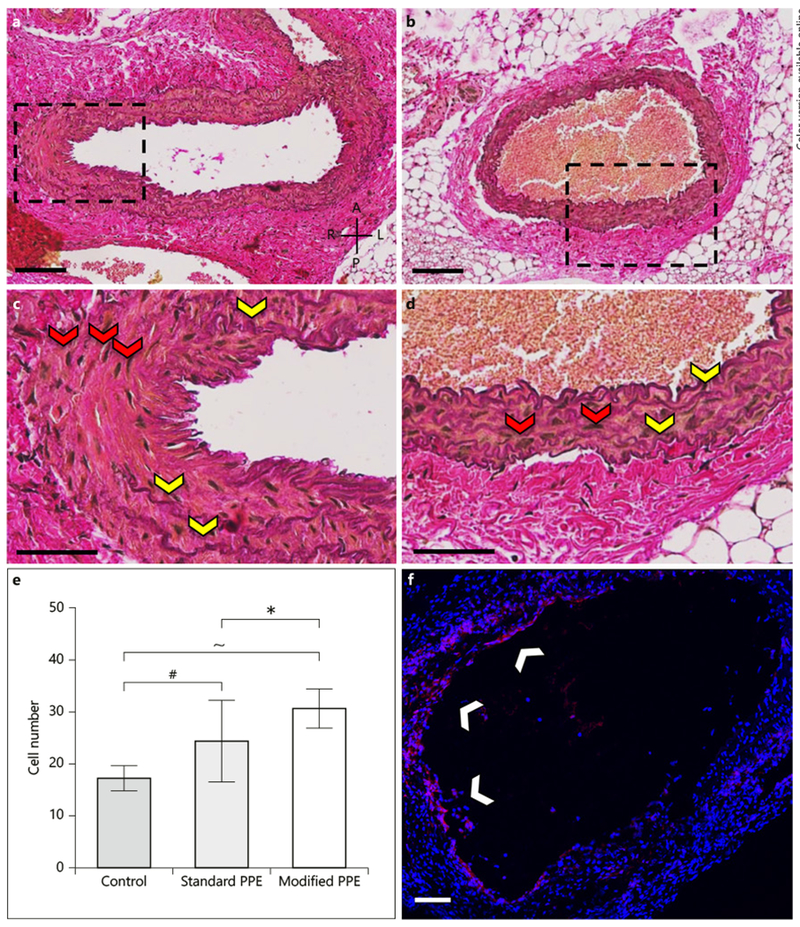
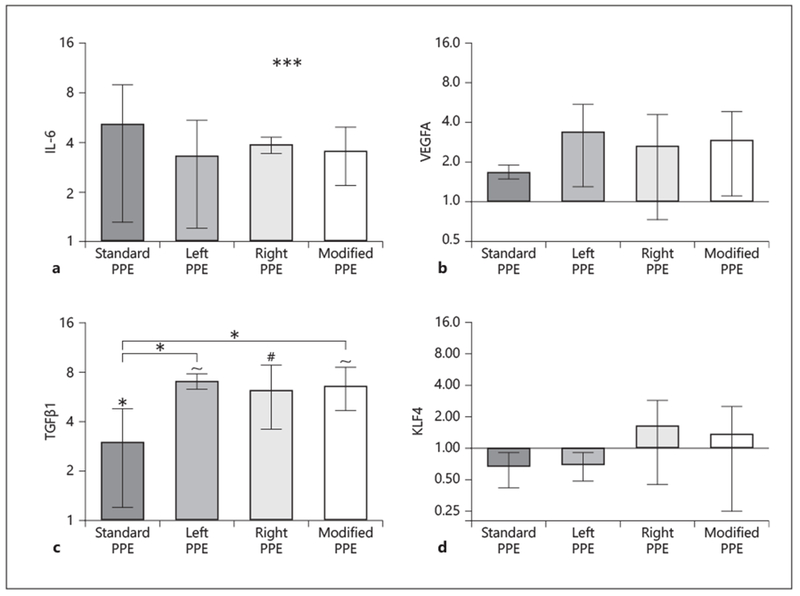
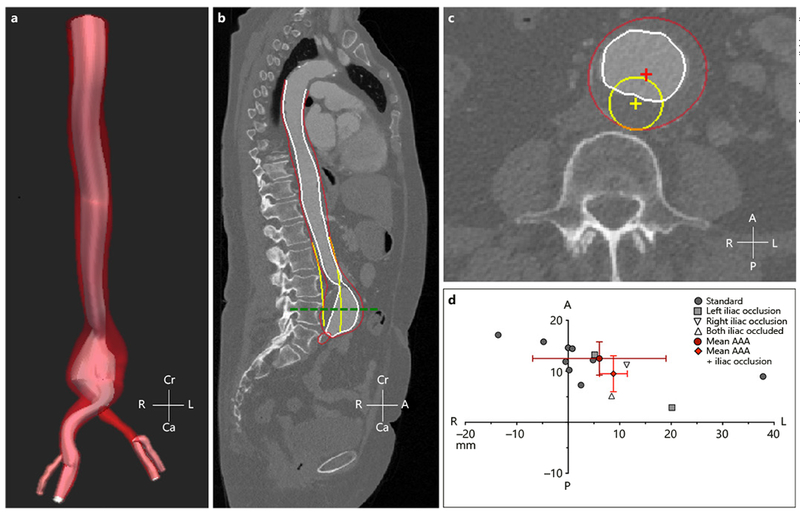
Reduced lower-limb blood flow has been shown to lead to asymmetrical abdominal aortic aneurysms (AAAs) but the mechanism of action is not fully understood. Therefore, small animal ultrasound (Vevo2100, FUJIFILM VisualSonics) was used to longitudinally study mice that underwent standard porcine pancreatic elastase (PPE) infusion (n = 5), and PPE infusion with modified 20% iliac artery stenosis in the left (n = 4) and right (n = 5) iliac arteries. Human AAA computed tomography images were obtained from patients with normal (n = 9) or stenosed left (n = 2), right (n = 1), and bilateral (n = 1) iliac arteries. We observed rapid early growth and rightward expansion (8/9 mice) in the modified PPE groups (p < 0.05), leading to slightly larger and asymmetric AAAs compared to the standard PPE group. Further examination showed a significant increase in TGFβ1 (p < 0.05) and cellular infiltration (p < 0.05) in the modified PPE group versus standard PPE mice. Congruent, yet variable, observations were made in human AAA patients with reduced iliac outflow compared to those with normal iliac outflow. Our results suggest that arterial stenosis at the time of aneurysm induction leads to faster AAA growth with aneurysm asymmetry and increased vascular inflammation after 8 weeks, indicating that moderate iliac stenosis may have upstream effects on AAA progression.
Keywords: Aneurysm; Asymmetry; Iliac artery; Murine.
© 2019 S. Karger AG, Basel.
Conflict of interest statement
Disclosure Statement
The authors have no conflict of interest to declare.
Figures
References
-
- Sampson UK, Norman PE, Fowkes FG, Aboyans V, Song Y, Harrell FE Jr, et al. Estimation of global and regional incidence and prevalence of abdominal aortic aneurysms 1990 to 2010. Glob Heart. 2014. March;9(1):159–70. - PubMed
-
- Sampson UKA, Norman PE, Fowkes FGR, Aboyans V, Song Y, Harrell FE Jr, et al. Global and regional burden of aortic dissection and aneurysms: mortality trends in 21 world regions, 1990 to 2010. Glob Heart. 2014 Mar; 9(1):171–80.e10. - PubMed
-
- Vardulaki KA, Prevost TC, Walker NM, Day NE, Wilmink AB, Quick CR, et al. Incidence among men of asymptomatic abdominal aortic aneurysms: estimates from 500 screen detected cases. J Med Screen. 1999;6(1):50–4. - PubMed
-
- Wassef M, Baxter BT, Chisholm RL, Dalman RL, Fillinger MF, Heinecke J, et al. Pathogenesis of abdominal aortic aneurysms: a multidisciplinary research program supported by the National Heart, Lung, and Blood Institute. J Vasc Surg. 2001. October;34(4):730–8. - PubMed
-
- Vollmar JF, Paes E, Pauschinger P, Henze E, Friesch A. Aortic aneurysms as late sequelae of above-knee amputation. Lancet. 1989. October; 2(8667):834–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
