

A cluster randomised trial of an intervention to increase the implementation of physical activity practices in secondary schools: study protocol for scaling up the Physical Activity 4 Everyone (PA4E1) program
- PMID: 31272421
- PMCID: PMC6610944
- DOI: 10.1186/s12889-019-6965-0
A cluster randomised trial of an intervention to increase the implementation of physical activity practices in secondary schools: study protocol for scaling up the Physical Activity 4 Everyone (PA4E1) program
Abstract
Background: The implementation of interventions at-scale is required to maximise population health benefits. 'Physical Activity 4 Everyone (PA4E1)' was a multi-component school-based program targeting adolescents attending secondary schools in low socio-economic areas. An efficacy trial of the intervention demonstrated an increase in students' mean minutes of moderate-to-vigorous physical activity (MVPA) per day and lower weight gain at low incremental cost. This study aims to assess the effectiveness and cost effectiveness of a multi-component implementation support intervention to improve implementation, at-scale, of the evidence based school physical activity (PA) practices of the PA4E1 program. Impact on student PA levels and adiposity will also be assessed, in addition to the cost of implementation.
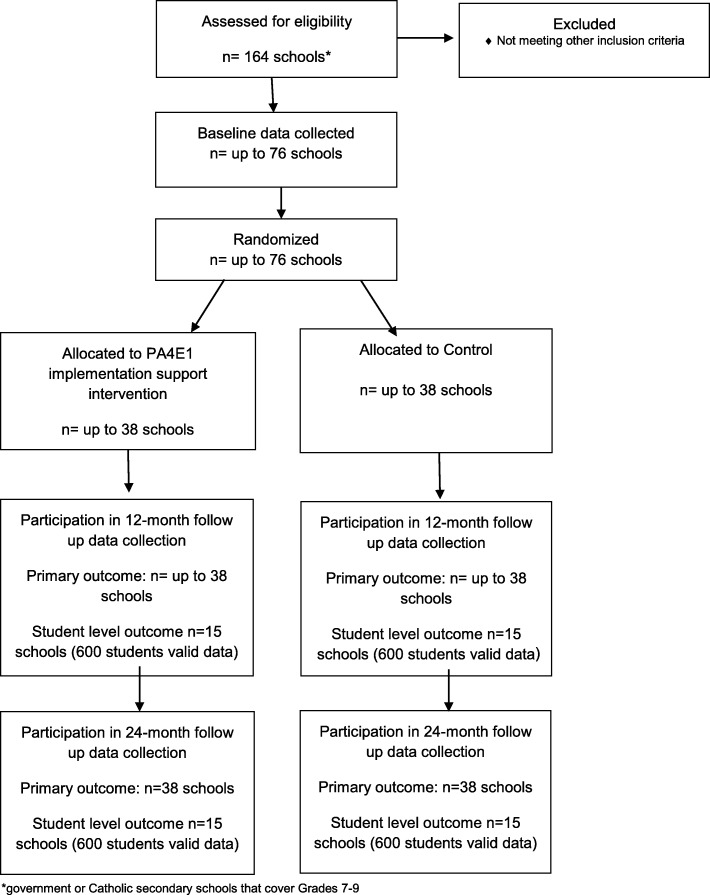
Methods: A cluster randomised controlled trial, utilising an effectiveness-implementation hybrid design, will be conducted in up to 76 secondary schools located in lower socio-economic areas across four health districts in New South Wales (NSW), Australia. Schools will be randomly allocated to a usual practice control arm or a multi-component implementation support intervention to embed the seven school PA practices of the PA4E1 program. The implementation support intervention incorporates seven strategies including executive support, in-School Champion, teacher training, resources, prompts, audit and feedback and access to an external Support Officer. The primary trial outcome will be the proportion of schools meeting at least four of the seven physical activity practices of the program, assessed via surveys with Head Physical Education teachers at 12 and 24-months. Secondary outcomes will be assessed via a nested evaluation of student PA and adiposity at 12-months (Grade 8 students) and 24 months (Grade 9 students) undertaken in 30 schools (15 per group). Resource use associated with the implementation intervention will be measured prospectively. Linear mixed effects regression models will assess program effects on the primary outcome at each follow-up period.
Discussion: This study is one of few evidence-based multi-component PA programs scaled-up to a large number of secondary schools and evaluated via randomised controlled trial. The use of implementation science theoretical frameworks to implement the evidence-based program and the rigorous evaluation design are strengths of the study.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12617000681358 registered 12th May 2017. Protocol Version 1.
Keywords: Adolescents; Physical activity; Randomised controlled trial, implementation, multi-component, scale-up; School.
Conflict of interest statement
Authors RS, EC, NN, LW, KG, MW, NE, AB and JW receive salary support from their respective Local Health Districts. Hunter New England Local Health District contributes funding to the project outlined in this protocol. None of these agencies were involved in the peer review of this grant. RS and NN are Associate Editors for BMC Public Health. All other authors declare that they have no competing interests.
References
-
- World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization; 2009. p. 62.
-
- Ding Ding, Lawson Kenny D, Kolbe-Alexander Tracy L, Finkelstein Eric A, Katzmarzyk Peter T, van Mechelen Willem, Pratt Michael. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. The Lancet. 2016;388(10051):1311–1324. - PubMed
-
- Biddle S. J. H., Asare M. Physical activity and mental health in children and adolescents: a review of reviews. British Journal of Sports Medicine. 2011;45(11):886–895. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
