

Lymph-node ratio is an important clinical determinant for selecting the appropriate adjuvant chemotherapy regimen for curative D2-resected gastric cancer
- PMID: 31273512
- PMCID: PMC11810259
- DOI: 10.1007/s00432-019-02963-7
Lymph-node ratio is an important clinical determinant for selecting the appropriate adjuvant chemotherapy regimen for curative D2-resected gastric cancer
Abstract
Purpose: Adjuvant chemotherapy for gastric cancer, particularly stage III, improves survival after curative D2 gastrectomy. We investigated the clinical value of the lymph-node ratio (LNR; number of metastatic lymph nodes/number of lymph nodes examined) for selecting the appropriate adjuvant chemotherapy regimen in patients with D2-resected stage II/III gastric cancer.
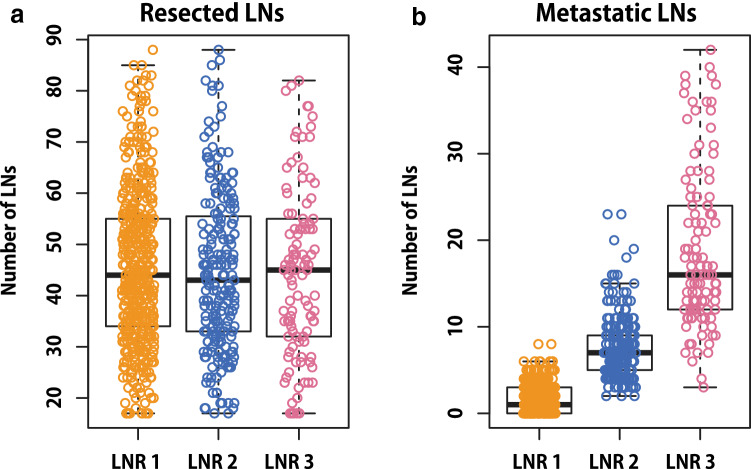
Methods: We reviewed the data of 819 patients who underwent curative D2 gastrectomy followed by adjuvant chemotherapy. Of them, 353 patients received platinum-based chemotherapy and 466 received TS-1. The patients were categorized into three groups according to their LNR (LNR 1, 0-0.1; LNR 2, > 0.1-0.25; and LNR 3, > 0.25), and their disease-free survival (DFS) was evaluated.
Results: The DFS curves of the patients were well separated according to stage and LNR. In multivariate analyses, an LNR > 0.1 was strongly associated with the 3-year DFS (hazard ratio 2.402, 95% confidence interval 1.607-3.590, P < 0.001). Platinum-based chemotherapy improved the 3-year DFS compared to TS-1 in patients with LNR 3 group in stage III gastric cancer (platinum vs. TS-1, median DFS 26.87 vs. 16.27 months, P = 0.028). An LNR > 0.1 was associated with benefiting from platinum-based adjuvant chemotherapy in stage III gastric cancer patients with lymphovascular invasion (platinum vs. TS-1, median DFS 47.57 vs. 21.77 months, P = 0.011).
Conclusions: The LNR can be used to select the appropriate adjuvant chemotherapy regimen for patients with D2-resected gastric cancer, particularly in stage III.
Keywords: Adjuvant chemotherapy; Gastrectomy; Gastric cancer; Lymph node.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures



References
-
- Bang YJ, Kim YW, Yang HK et al (2012) Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet 379:315–321. 10.1016/S0140-6736(11)61873-4 - PubMed
-
- Bilici A, Seker M, Ustaalioglu BB et al (2010) Determining of metastatic lymph node ratio in patients who underwent D2 dissection for gastric cancer. Med Oncol 27:975–984. 10.1007/s12032-009-9319-4 - PubMed
-
- Cheong JH, Yang HK, Kim H et al (2018) Predictive test for chemotherapy response in resectable gastric cancer: a multi-cohort, retrospective analysis. Lancet Oncol 19:629–638. 10.1016/S1470-2045(18)30108-6 - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
