

Chlorambucil targets BRCA1/2-deficient tumours and counteracts PARP inhibitor resistance
- PMID: 31273933
- PMCID: PMC6609913
- DOI: 10.15252/emmm.201809982
Chlorambucil targets BRCA1/2-deficient tumours and counteracts PARP inhibitor resistance
Abstract
Due to compromised homologous recombination (HR) repair, BRCA1- and BRCA2-mutated tumours accumulate DNA damage and genomic rearrangements conducive of tumour progression. To identify drugs that target specifically BRCA2-deficient cells, we screened a chemical library containing compounds in clinical use. The top hit was chlorambucil, a bifunctional alkylating agent used for the treatment of chronic lymphocytic leukaemia (CLL). We establish that chlorambucil is specifically toxic to BRCA1/2-deficient cells, including olaparib-resistant and cisplatin-resistant ones, suggesting the potential clinical use of chlorambucil against disease which has become resistant to these drugs. Additionally, chlorambucil eradicates BRCA2-deficient xenografts and inhibits growth of olaparib-resistant patient-derived tumour xenografts (PDTXs). We demonstrate that chlorambucil inflicts replication-associated DNA double-strand breaks (DSBs), similarly to cisplatin, and we identify ATR, FANCD2 and the SNM1A nuclease as determinants of sensitivity to both drugs. Importantly, chlorambucil is substantially less toxic to normal cells and tissues in vitro and in vivo relative to cisplatin. Because chlorambucil and cisplatin are equally effective inhibitors of BRCA2-compromised tumours, our results indicate that chlorambucil has a higher therapeutic index than cisplatin in targeting BRCA-deficient tumours.
Keywords: BRCA1; BRCA2; DNA damage responses; alkylating agents; cisplatin.
© 2019 The Authors. Published under the terms of the CC BY 4.0 license.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

- A
Dose‐dependent viability assays of BRCA2‐proficient (+BRCA2) or BRCA2‐deficient (−BRCA2) human DLD1 cells treated with drugs at the indicated concentrations for 6 days.
- B
Human spheroids established from BRCA2‐proficient (+BRCA2) or BRCA2‐deficient (−BRCA2) DLD1 cells were incubated with 1.25 µM olaparib or 0.5 µM chlorambucil over the indicated period of time.

- A
Dose‐dependent viability assays of BRCA1‐proficient (+BRCA1) or BRCA2‐deficient (−BRCA1) human RPE1‐hTERT and TP53‐deleted cells treated with drugs at the indicated concentrations for 6 days.
- B, C
Dose‐dependent viability assays of Brca1 +/+ and Brca1 −/− mouse mammary tumour‐derived cell lines treated with drugs at the indicated concentrations for 6 days.
- A
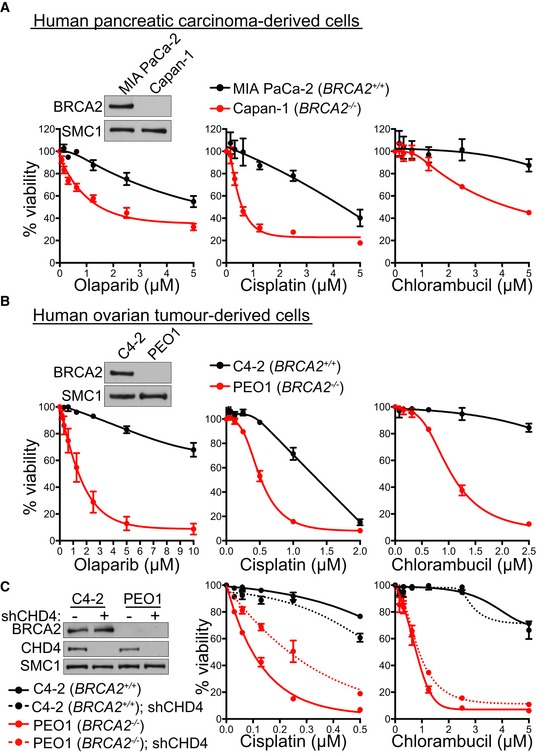
Dose‐dependent viability assays of BRCA2‐deficient (Capan‐1) or BRCA2‐proficient (MIA PaCa‐2) human pancreatic carcinoma‐derived cells treated with drugs at the indicated concentrations for 6 days.
- B
Dose‐dependent viability assays of BRCA2‐deficient (PEO1) or BRCA2‐proficient (C4‐2) human ovarian tumour‐derived cells treated with drugs at the indicated concentrations for 6 days.
- C
BRCA2‐deficient (PEO1) or BRCA2‐proficient (C4‐2) human ovarian tumour‐derived cells were infected with lentiviruses expressing control or CHD4 shRNAs, followed by selection with puromycin for 72 h. Dose‐dependent viability assays were performed on cells treated with drugs at the indicated concentrations for 6 days.

- A
BRCA2‐proficient (+BRCA2) or BRCA2‐deficient (−BRCA2) human DLD1 cells were incubated with 1 µM chlorambucil (Chl). Whole‐cell extracts prepared at the indicated time points during treatment were immunoblotted as shown. GAPDH was used as a loading control.
- B
Quantification of chromosome aberrations and chromatid/chromosome break frequencies in BRCA2‐proficient (+BRCA2) or BRCA2‐deficient (−BRCA2) human DLD1 cells incubated with 1 μM chlorambucil or 1 µM cisplatin for 72 h. Data were obtained from three independent experiments and normalised to untreated controls. A minimum of 60 Giemsa‐stained metaphases were analysed for each sample. Cis, cisplatin; Chl, chlorambucil.
- C
Quantification of G2/M cell frequency relative to solvent control, using FACS analyses of cells incubated with 1 μM chlorambucil or 1 µM cisplatin for 48 h. Cis, cisplatin; Chl, chlorambucil.
- D, E
Human H1299 cells were treated with control (CTR) or indicated siRNAs 2 days before drugs were added to the media for dose‐dependent viability assays. Cell extracts prepared at the time of drug addition were immunoblotted as indicated. SMC1 was used as a loading control.

- A, B
Nude mice (nu/nu) were injected subcutaneously with 5 × 106 human DLD1 cells, BRCA2‐proficient (A) or BRCA2‐deficient (B). Tumour‐bearing mice were treated with 3 mg/kg daily chlorambucil administered intraperitoneally (i.p.) for a total of 10 days. Tumour weight was determined on the indicated days after initiation of the treatment.
- C
PDTCs derived from breast cancer samples as previously described (Bruna et al, 2016) were treated with chlorambucil at the indicated doses. Cell survival is represented relative to DMSO control. AB521, ER‐negative tumour, no BRCA1 alteration; STG201, tumour with BRCA1 promoter methylation and loss of BRCA1 expression; VHIO179, tumour with BRCA1 germline mutation and MAD2L2 inactivating mutation (olaparib‐resistant);
http://caldaslab.cruk.cam.ac.uk/bcape/ . - D
CB17/SCID mice were injected intramuscularly with 5 × 106 human BRCA2‐deficient HCT116 cells. Tumour‐bearing mice were treated on the indicated days with chlorambucil or cisplatin administered intraperitoneally (i.p.), or talazoparib administered orally (o.s.) Tumour volume was measured on the indicated days after treatment initiation and was expressed relative to tumour volume at the beginning of treatment (day 1). Scale bar, 40 µm.

- A
Wild‐type Balb/c mice were injected intraperitoneally with solvent (daily) or 3 mg/kg chlorambucil (daily for 5 days) or 3.3 mg/kg cisplatin (daily for 3 days). Uptake of the apoptosis tracer 99mTc‐Duramycin 2 h after intravenous injection was quantified in selected organs using SPECT imaging in the indicated organs. Representative maximum intensity partial projections showing tracer distribution are shown.
- B
Immunohistochemical analyses of γH2AX staining in organs from mice treated as in (A). Scale bar, 25 µm.
References
-
- Ang JE, Gourley C, Powell CB, High H, Shapira‐Frommer R, Castonguay V, De Greve J, Atkinson T, Yap TA, Sandhu S et al (2013) Efficacy of chemotherapy in BRCA1/2 mutation carrier ovarian cancer in the setting of PARP inhibitor resistance: a multi‐institutional study. Clin Cancer Res 19: 5485–5493 - PubMed
-
- Barker GH, Wiltshaw E (1981) Randomised trial comparing low‐dose cisplatin and chlorambucil with low‐dose cisplatin, chlorambucil, and doxorubicin in advanced ovarian carcinoma. Lancet 1: 747–750 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
