

Computer Vision Analysis of Intraoperative Video: Automated Recognition of Operative Steps in Laparoscopic Sleeve Gastrectomy
- PMID: 31274652
- PMCID: PMC7216040
- DOI: 10.1097/SLA.0000000000003460
Computer Vision Analysis of Intraoperative Video: Automated Recognition of Operative Steps in Laparoscopic Sleeve Gastrectomy
Abstract
Objective(s): To develop and assess AI algorithms to identify operative steps in laparoscopic sleeve gastrectomy (LSG).
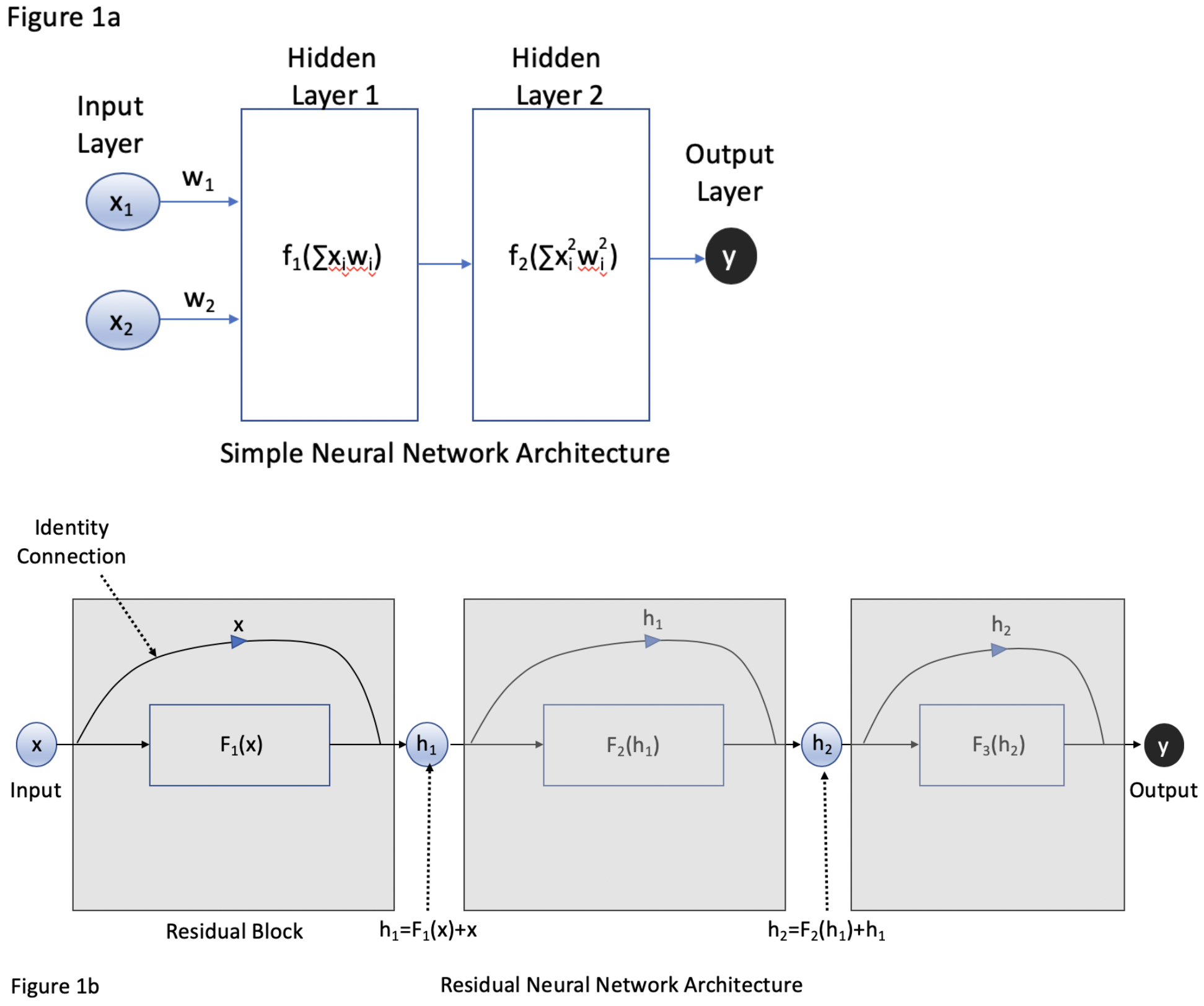
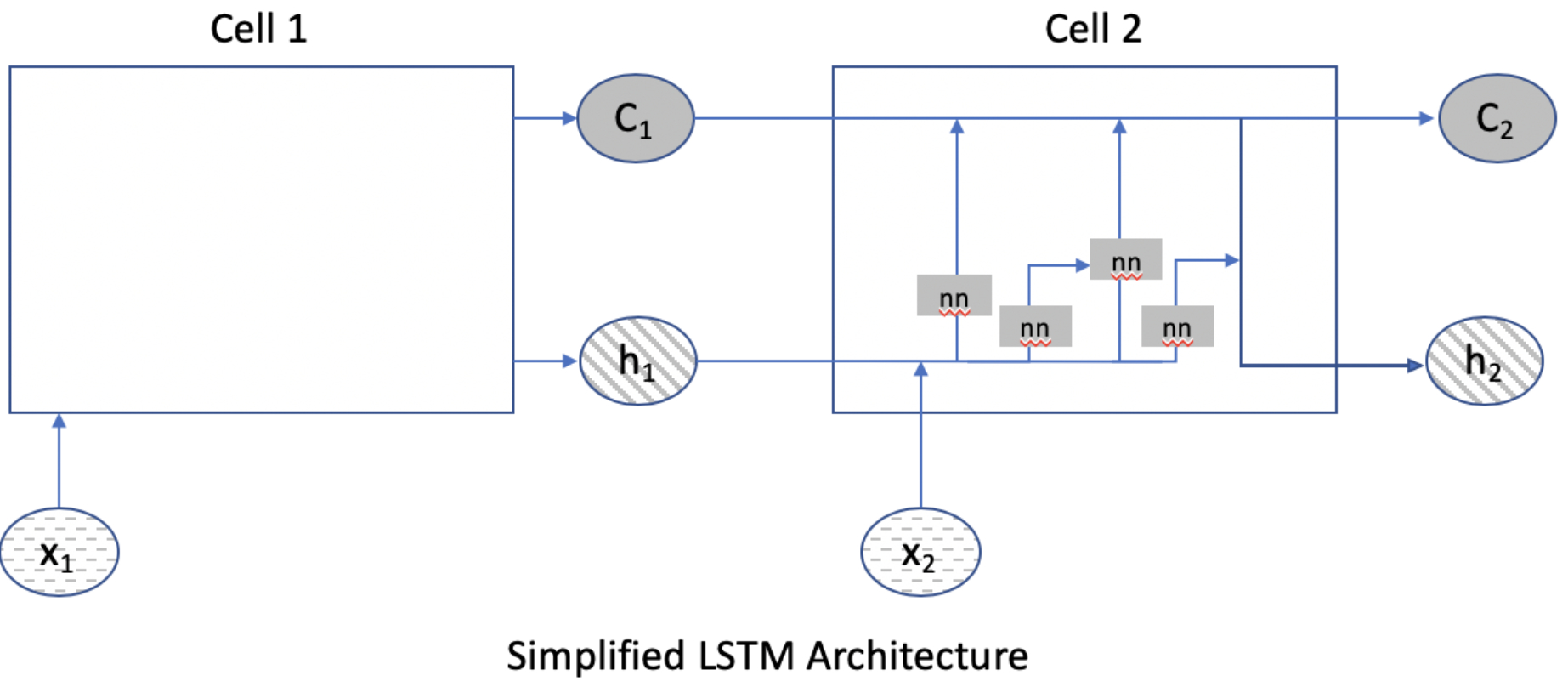
Background: Computer vision, a form of artificial intelligence (AI), allows for quantitative analysis of video by computers for identification of objects and patterns, such as in autonomous driving.
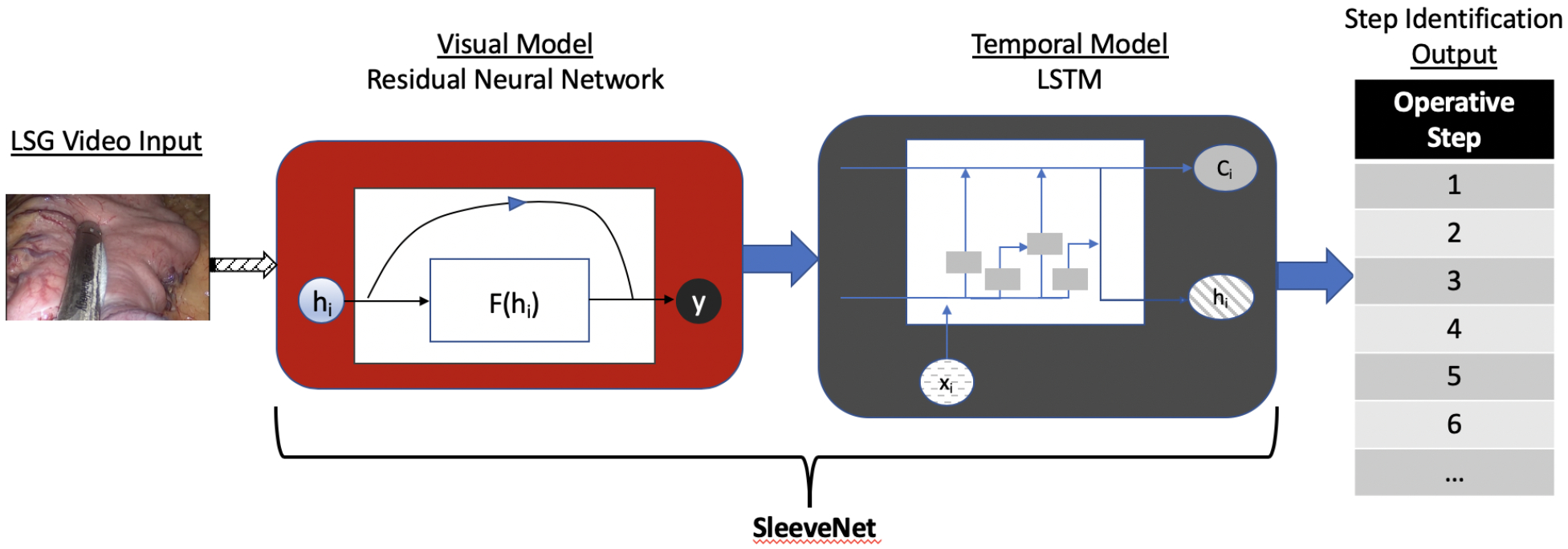
Methods: Intraoperative video from LSG from an academic institution was annotated by 2 fellowship-trained, board-certified bariatric surgeons. Videos were segmented into the following steps: 1) port placement, 2) liver retraction, 3) liver biopsy, 4) gastrocolic ligament dissection, 5) stapling of the stomach, 6) bagging specimen, and 7) final inspection of staple line. Deep neural networks were used to analyze videos. Accuracy of operative step identification by the AI was determined by comparing to surgeon annotations.
Results: Eighty-eight cases of LSG were analyzed. A random 70% sample of these clips was used to train the AI and 30% to test the AI's performance. Mean concordance correlation coefficient for human annotators was 0.862, suggesting excellent agreement. Mean (±SD) accuracy of the AI in identifying operative steps in the test set was 82% ± 4% with a maximum of 85.6%.
Conclusions: AI can extract quantitative surgical data from video with 85.6% accuracy. This suggests operative video could be used as a quantitative data source for research in intraoperative clinical decision support, risk prediction, or outcomes studies.
Figures
References
-
- Hu YY, Mazer LM, Yule SJ, et al. Complementing Operating Room Teaching With Video-Based Coaching. JAMA Surg 2017; 152(4):318–325. - PubMed
-
- Greenberg CC, Ghousseini HN, Pavuluri Quamme SR, et al. A Statewide Surgical Coaching Program Provides Opportunity for Continuous Professional Development. Ann Surg 2018; 267(5):868–873. - PubMed
-
- Deal SB, Stefanidis D, Telem D, et al. Evaluation of crowd-sourced assessment of the critical view of safety in laparoscopic cholecystectomy. Surgical Endoscopy 2017:1–7. - PubMed
-
- Franke S, Meixensberger J, Neumuth T. Multi-perspective workflow modeling for online surgical situation models. J Biomed Inform 2015; 54:158–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
