

Left Subclavian Artery Revascularization for Delayed Paralysis after Thoracic Endovascular Aortic Repair
- PMID: 31275481
- PMCID: PMC6600088
- DOI: 10.3400/avd.cr.18-00158
Left Subclavian Artery Revascularization for Delayed Paralysis after Thoracic Endovascular Aortic Repair
Abstract
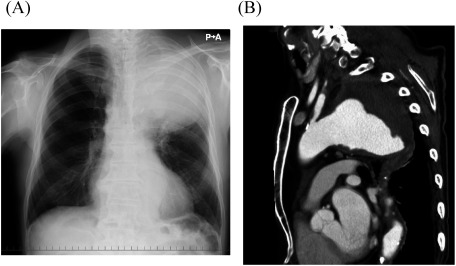
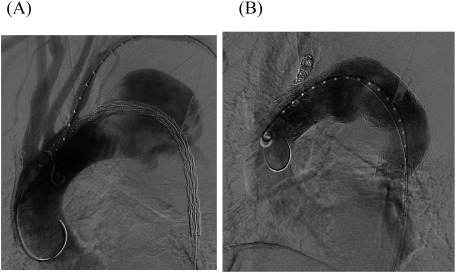
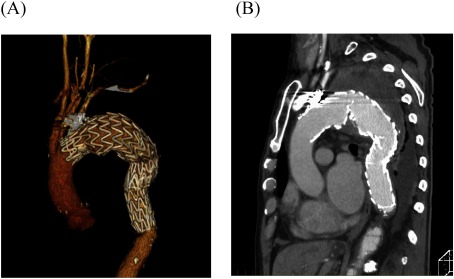
Spinal cord ischemia (SCI) is a devastating complication following thoracic endovascular aortic repair (TEVAR). A man with a ruptured thoracic aortic aneurysm (TAA) was transferred to our hospital. Emergency TEVAR, with left subclavian artery (LSA) coverage, was performed for the ruptured TAA. On postoperative day two, the patient had incomplete paralysis in his legs, presumably caused by SCI. We performed LSA revascularization (LSAR) to provide blood supply to the spinal cord; his paralysis improved and almost resolved after surgery. To our knowledge, this is the first report on LSAR's efficacy for delayed paraplegia due to SCI.
Keywords: delayed paralysis; left subclavian artery revascularization; thoracic endovascular aortic repair.
Conflict of interest statement
Disclosure StatementNone declared.
Figures
References
-
- Griepp RB, Griepp EB. Spinal cord perfusion and protection during descending thoracic and thoracoabdominal aortic surgery: the collateral network concept. Ann Thorac Surg 2007; 83: S865-9. - PubMed
-
- Acher C, Acher CW, Marks E, et al. Intraoperative neuroprotective interventions prevent spinal cord ischemia and injury in thoracic endovascular aortic repair. J Vasc Surg 2016; 63: 1458-65. - PubMed
-
- Amato ACM, Stolf NAG. Anatomy of spinal blood supply. J Vasc Bras 2015; 14: 248-52.
-
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010; 121: e266-369. - PubMed