

Long-term status of predicted body fat percentage, body mass index and other anthropometric factors with risk of colorectal carcinoma: Two large prospective cohort studies in the US
- PMID: 31276608
- PMCID: PMC7282530
- DOI: 10.1002/ijc.32553
Long-term status of predicted body fat percentage, body mass index and other anthropometric factors with risk of colorectal carcinoma: Two large prospective cohort studies in the US
Abstract
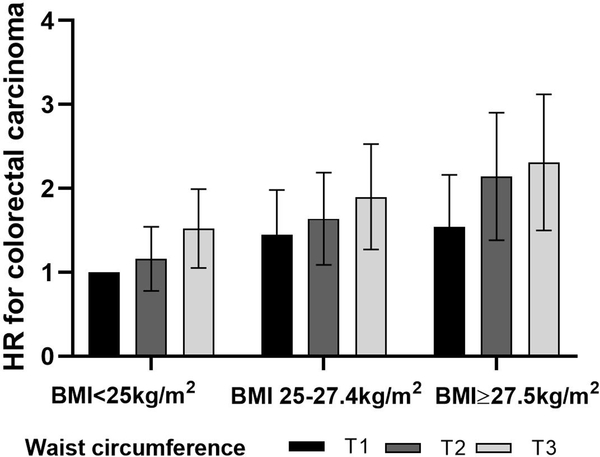
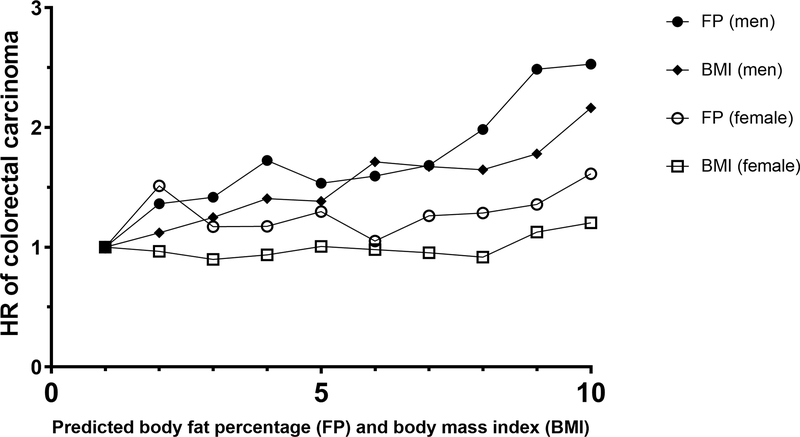
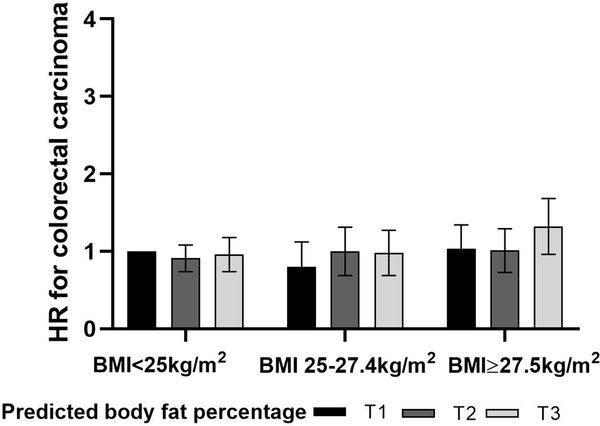
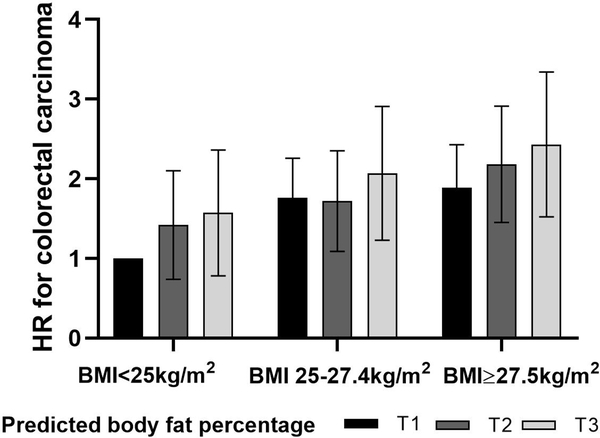
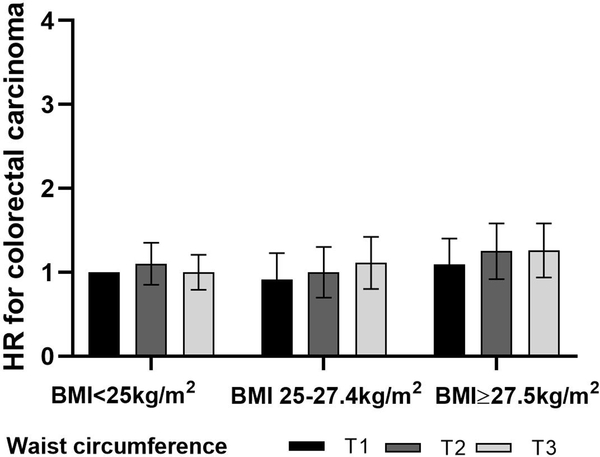
Anthropometric measurements, such as body mass index (BMI), waist circumference, and body fat percentage, have been used as indicators of obesity. Despite evidence that excess body fat is a risk factor for colorectal carcinoma (CRC), the magnitude of the association of BMI and other obesity indicators with the long-term risk of CRC remains unclear. Utilizing a Cox proportional hazards regression model, we examined differential associations between predicted body fat percentage and BMI with the risk of CRC (n = 2,017). The associations between CRC incidence and different adiposity measurements were also assessed. Predicted body fat percentage had a similar increased risk of CRC risk as BMI. In multivariable-adjusted analyses, the hazard ratio for CRC in the second to fifth quintiles (compared to the first quintile) of predicted body fat percentage were 1.32, 1.31, 1.53 and 2.09 for men (ptrend < 0.001) and 0.91, 0.90, 0.98 and 1.15 for women (ptrend = 0.03). Among various anthropometric measurements, predicted fat mass and waist circumference were slightly more strongly associated with CRC risk than BMI. In conclusion, the novel anthropometric prediction equations provided further evidence that a greater amount of body fat might contribute to CRC risk in both sexes. An innovative approach enabled us to estimate the susceptibilities of specific body composition with CRC risk, in an inexpensive and minimally invasive manner. Furthermore, the typically used measures of BMI and waist circumference are robust measures of adiposity to predict cancer risk in a relatively healthy population.
Keywords: body composition; body fat percentage; colorectal cancer; obesity; visceral adiposity.
© 2019 UICC.
Conflict of interest statement
Figures
Similar articles
-
A Prospective Investigation of Body Size, Body Fat Composition and Colorectal Cancer Risk in the UK Biobank.Sci Rep. 2017 Dec 19;7(1):17807. doi: 10.1038/s41598-017-17997-5. Sci Rep. 2017. PMID: 29259258 Free PMC article.
-
Long-term status and change of body fat distribution, and risk of colorectal cancer: a prospective cohort study.Int J Epidemiol. 2016 Jun;45(3):871-83. doi: 10.1093/ije/dyv177. Epub 2015 Sep 24. Int J Epidemiol. 2016. PMID: 26403814 Free PMC article.
-
The prediction of colorectal cancer using anthropometric measures: A Swedish population-based cohort study with 22 years of follow-up.United European Gastroenterol J. 2019 Nov;7(9):1250-1260. doi: 10.1177/2050640619854278. Epub 2019 May 24. United European Gastroenterol J. 2019. PMID: 31700638 Free PMC article.
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
-
Anthropometric and adiposity indicators and risk of type 2 diabetes: systematic review and dose-response meta-analysis of cohort studies.BMJ. 2022 Jan 18;376:e067516. doi: 10.1136/bmj-2021-067516. BMJ. 2022. PMID: 35042741 Free PMC article.
Cited by
-
Association of Adiponectin and Vitamin D With Tumor Infiltrating Lymphocytes and Survival in Stage III Colon Cancer.JNCI Cancer Spectr. 2021 Jul 23;5(5):pkab070. doi: 10.1093/jncics/pkab070. eCollection 2021 Oct. JNCI Cancer Spectr. 2021. PMID: 34485815 Free PMC article. Clinical Trial.
-
Adiposity and risks of gastrointestinal cancers: A 10-year prospective study of 0.5 million Chinese adults.Int J Cancer. 2025 Jun 1;156(11):2094-2106. doi: 10.1002/ijc.35303. Epub 2024 Dec 31. Int J Cancer. 2025. PMID: 39737804 Free PMC article.
-
Associations of Albumin and BMI with Colorectal Cancer Risk in the Southern Community Cohort Study: a Prospective Cohort Study.J Racial Ethn Health Disparities. 2024 Dec;11(6):3445-3456. doi: 10.1007/s40615-023-01797-x. Epub 2023 Sep 21. J Racial Ethn Health Disparities. 2024. PMID: 37733284
-
Body mass index, weight change, and cancer prognosis: a meta-analysis and systematic review of 73 cohort studies.ESMO Open. 2024 Mar;9(3):102241. doi: 10.1016/j.esmoop.2024.102241. Epub 2024 Mar 4. ESMO Open. 2024. PMID: 38442453 Free PMC article.
-
The perils of using predicted values in place of observed covariates: an example of predicted values of body composition and mortality risk.Am J Clin Nutr. 2021 Aug 2;114(2):661-668. doi: 10.1093/ajcn/nqab074. Am J Clin Nutr. 2021. PMID: 33831946 Free PMC article.
References
-
- Flegal KM, Carroll MD, Kuczmarski RJ, Johnson CL. Overweight and obesity in the United States: prevalence and trends, 1960–1994. Int J Obes Relat Metab Disord 1998;22:39–47. - PubMed
-
- Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA 2012;307:491–7. - PubMed
-
- Roberto CA, Swinburn B, Hawkes C, Huang TT-K, Costa SA, Ashe M, Zwicker L, Cawley JH, Brownell KD. Patchy progress on obesity prevention: emerging examples, entrenched barriers, and new thinking. Lancet (London, England) 2015;385:2400–9. - PubMed
-
- Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 2008;371:569–78. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
