

The outcome of Bishop-Koop procedure compared to divided stoma in neonates with meconium ileus, congenital intestinal atresia and necrotizing enterocolitis
- PMID: 31277168
- PMCID: PMC6635230
- DOI: 10.1097/MD.0000000000016304
The outcome of Bishop-Koop procedure compared to divided stoma in neonates with meconium ileus, congenital intestinal atresia and necrotizing enterocolitis
Abstract
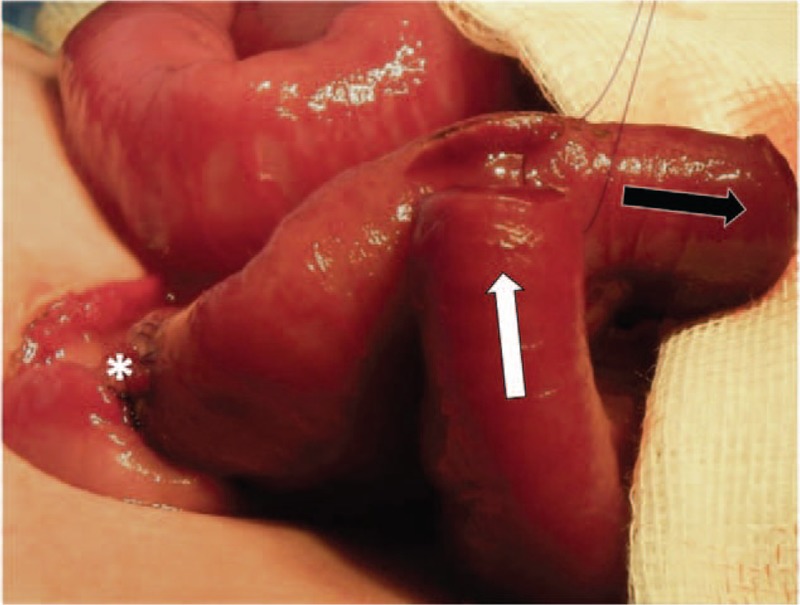
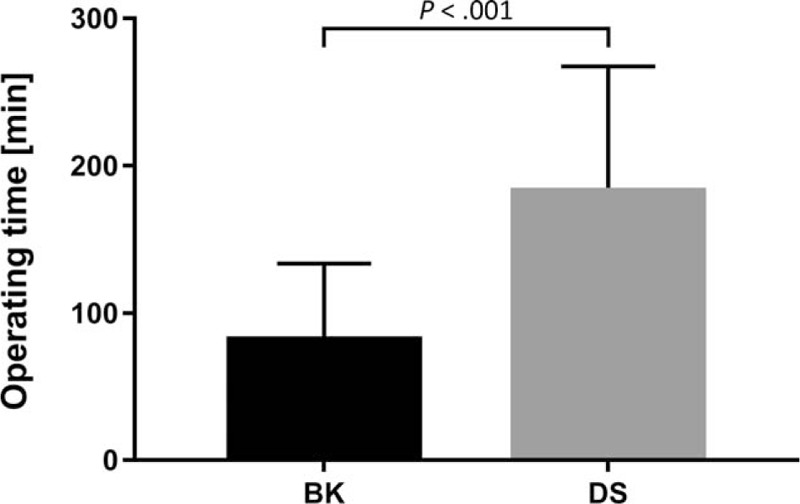
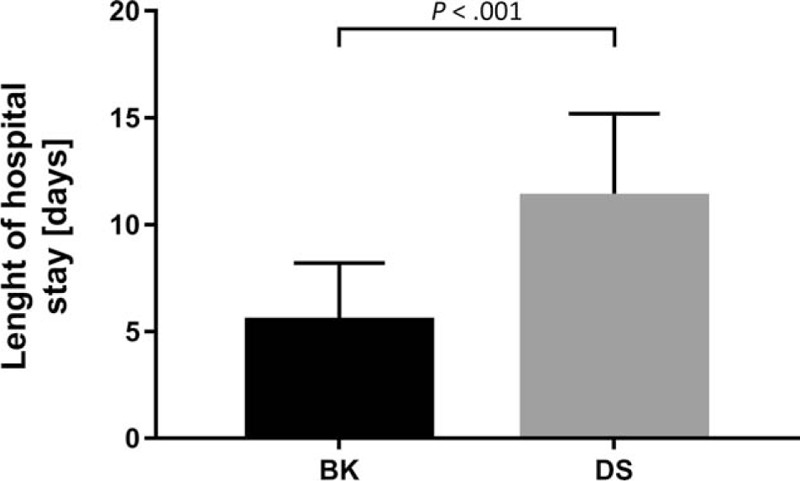
To determine the potential value and suitability of Bishop-Koop procedure (BK) compared to divided stoma (DS) in neonates with meconium ileus (MI), congenital intestinal atresia (CIA), and necrotizing enterocolitis (NEC).A retrospective data collection from 2000 to 2019 on neonates undergoing BK and DS formation and closure for MI, CIA, and NEC was conducted. Ostomy related complications following both procedures were analyzed.One hundred two consecutive patients managed with a BK (n = 57, 55.8%) and DS (n = 45, 44.2%) for MI (n = 38, 37.2%), CIA (n = 31, 30.5%), and NEC (n = 33, 32.3%) were analyzed. Mean operating time for ostomy creation did not differ significantly between BK and DS groups (156 ± 54 vs 135 ± 66.8 min, P = .08). The prevalence of stoma-related complications following BK and DS formation was 8.7% and 31.1%, respectively (P = .005). The complication rate after BK and DS closure was 3.5% and 6.7%, respectively (P = .65). The operating time for ostomy reversal and length of hospital stay after stoma closure were significantly shorter in BK group (82.2 ± 51.4 vs 183 ± 84.5 min and 5.5 ± 2.7 vs 11.3 ± 3.9 days, P < .001).BK procedure is safe, reliable, and suitable technique in neonatal surgery with low complications rate following ostomy creation as well as shorter operating time and length of hospital stay after ostomy closure compared to DS ostomies. Surgeons should keep this technique as an alternative approach in their repertoire.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
BISHOP-KOOP OSTOMY REVISITED: A "TEST-DRIVE" INTESTINAL DIVERSION FOR CHILDREN WITH SUSPECTED BOWEL DYSMOTILITY.Arq Bras Cir Dig. 2023 Mar 20;36:e1722. doi: 10.1590/0102-672020230002e1722. eCollection 2023. Arq Bras Cir Dig. 2023. PMID: 36946847 Free PMC article. Review.
-
[Application of Bishop-Koop stoma in refractory congenital intestinal atresia].Zhonghua Wei Chang Wai Ke Za Zhi. 2016 Oct 25;19(10):1154-1159. Zhonghua Wei Chang Wai Ke Za Zhi. 2016. PMID: 27781254 Chinese.
-
Optimal Timing of Stoma Closure in Premature Infants Affected by Necrotizing Enterocolitis.J Surg Res. 2025 Jan;305:265-274. doi: 10.1016/j.jss.2024.11.033. Epub 2024 Dec 27. J Surg Res. 2025. PMID: 39937559
-
Timing and outcome of stoma closure in very low birth weight infants with surgical intestinal disorders.Surg Today. 2017 Aug;47(8):1001-1006. doi: 10.1007/s00595-017-1498-6. Epub 2017 Feb 28. Surg Today. 2017. PMID: 28247106
-
The surgical management of necrotising enterocolitis (NEC).Early Hum Dev. 2016 Jun;97:25-8. doi: 10.1016/j.earlhumdev.2016.03.002. Epub 2016 Mar 29. Early Hum Dev. 2016. PMID: 27032753 Review.
Cited by
-
A retrospective cohort study of the application of Santulli enterostomy in neonatal necrotizing enterocolitis.Sci Rep. 2025 Jan 9;15(1):1475. doi: 10.1038/s41598-024-84384-2. Sci Rep. 2025. PMID: 39789045 Free PMC article.
-
Santulli Procedure Revisited in Congenital Intestinal Malformations and Postnatal Intestinal Injuries: Preliminary Report of Experience.Children (Basel). 2022 Jan 7;9(1):84. doi: 10.3390/children9010084. Children (Basel). 2022. PMID: 35053709 Free PMC article.
-
Outcomes of enterotomy and bowel irrigation for simple meconium ileus: case series and literature review.Pediatr Surg Int. 2025 May 9;41(1):133. doi: 10.1007/s00383-025-06028-4. Pediatr Surg Int. 2025. PMID: 40343521 Review.
-
BISHOP-KOOP OSTOMY REVISITED: A "TEST-DRIVE" INTESTINAL DIVERSION FOR CHILDREN WITH SUSPECTED BOWEL DYSMOTILITY.Arq Bras Cir Dig. 2023 Mar 20;36:e1722. doi: 10.1590/0102-672020230002e1722. eCollection 2023. Arq Bras Cir Dig. 2023. PMID: 36946847 Free PMC article. Review.
-
[Effect of low-dose dopamine adjuvant therapy on inflammatory factors and prognosis in preterm infants with necrotizing enterocolitis].Zhongguo Dang Dai Er Ke Za Zhi. 2020 Feb;22(2):136-140. doi: 10.7499/j.issn.1008-8830.2020.02.010. Zhongguo Dang Dai Er Ke Za Zhi. 2020. PMID: 32051080 Free PMC article. Chinese.
References
-
- Jawaheer J, Khalil B, Plummer T, et al. Primary resection and anastomosis for complicated meconium ileus: a safe procedure? Pediatr Surg Int 2007;23:1091–3. - PubMed
-
- Hillyer MM, Baxter KJ, Clifton MS, et al. Primary versus secondary anastomosis in intestinal atresia. J Pediatr Surg 2018;54:417–22. - PubMed
-
- Stollman TH, de Blaauw I, Wijnen MH, et al. Decreased mortality but increased morbidity in neonates with jejunoileal atresia; a study of 114 cases over a 34-year period. J Pediatr Surg 2009;44:217–21. - PubMed
-
- Singh M, Owen A, Gull S, et al. Surgery for intestinal perforation in preterm neonates: anastomosis vs stoma. J Pediatr Surg 2006;41:725–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
