

Intrahepatic mass-forming cholangiocarcinoma growing in a giant hepatic hemangioma: A case report
- PMID: 31277198
- PMCID: PMC6635132
- DOI: 10.1097/MD.0000000000016410
Intrahepatic mass-forming cholangiocarcinoma growing in a giant hepatic hemangioma: A case report
Abstract
Rationale: Hepatic hemangioma (HH) is a common benign tumor with a high number of normal or abnormal blood vessels. Intrahepatic cholangiocarcinoma (ICC) is a relatively common malignant primary hepatic carcinoma (10%-15%) with high incidence rate and high fatality, yet low discovery rate in the early stages. Ultrasonography (US), computed tomography, and magnetic resonance imaging (MRI) are frequently used and indispensable imaging techniques for the diagnosis of hepatic lesions. It is possible to differentiate a liver lesion from HH with high accuracy owing to their different patterns and hemodynamic characteristics.
Patient concerns: A 59-year-old Asian woman was referred to hospital for a hepatic mass, which was 9.0 × 6.5 cm in size, The patient was tested positive for hepatitis B antigen but negative for serum alpha-fetoprotein and carbohydrate antigen 199 and had a slightly elevated carcinoembryonic antigen level (3.56 ng/ml).
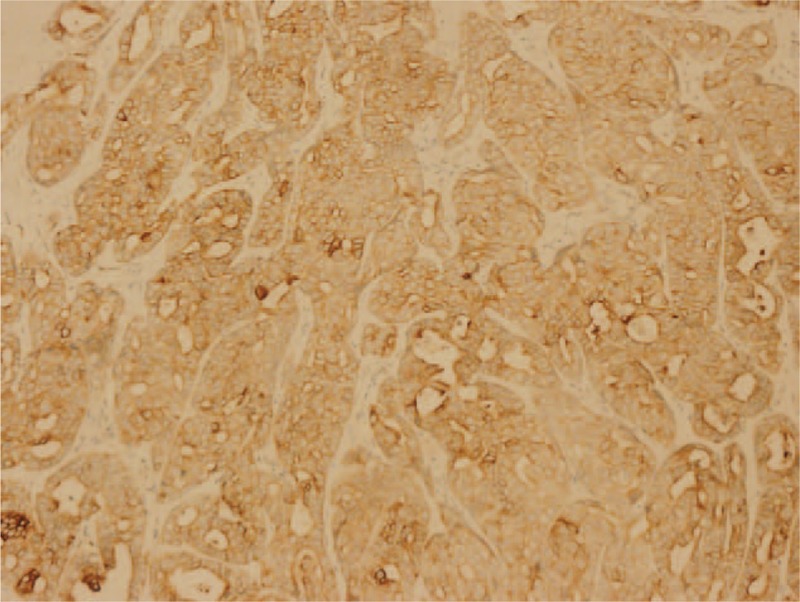
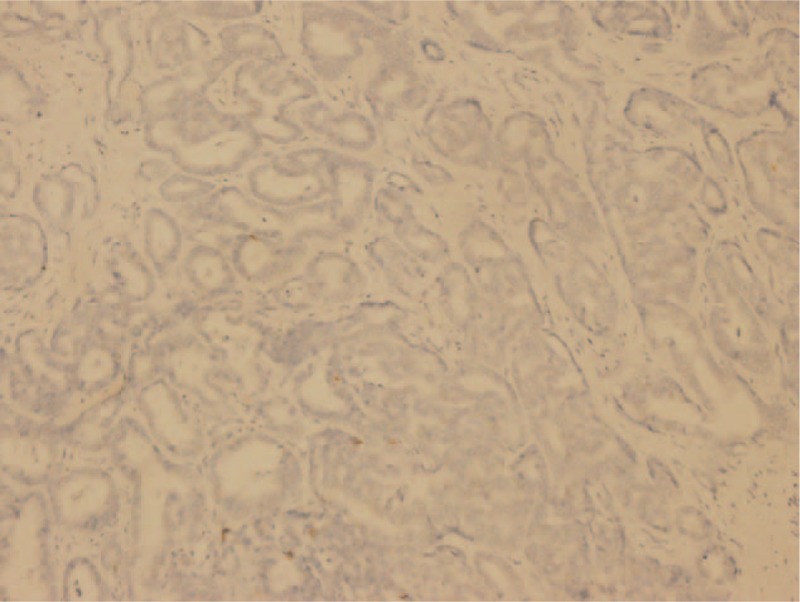
Diagnosis: Liver US and MRI were performed. Grey-scale US revealed a huge heterogeneous mass on the right lobe with a point and line-like blood flow signal on Doppler US. Dynamic contrast-enhanced MRI showed heterogeneous annular nodular enhancement in the arterial phase. An initial diagnosis of HH was made based on the clinical history and imaging results; however, histopathologic examination of the liver lesions revealed modest to severe atypical hyperplasia of intrahepatic bile duct epithelium, cancerization, and mid to high differentiated mass-forming type cholangiocarcinoma combined with focal organized hemangioma.
Interventions: The intrahepatic mass-forming cholangiocarcinoma (IMCC) lesion was considered a focal organization of hemangioma during operation and was surgically removed. No routine chemotherapy was performed after the operation.
Outcomes: The IMCC recurred 23 months after surgery, with elevated serum CA19-9 and CA125. Liver damage was evident, and the patient developed jaundice. The patient was discharged without active treatment and died in 4 months.
Lessons: Although preoperative imaging of focal hepatic lesions is indispensable, intraoperative frozen section analysis and histopathological examination remain essential for definitive diagnosis. This is particularly important for high-risk patients and those with suspected malignancy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures










Similar articles
-
Atypical hemangioma mimicking mixed hepatocellular cholangiocarcinoma: Case report.Medicine (Baltimore). 2017 Dec;96(50):e9192. doi: 10.1097/MD.0000000000009192. Medicine (Baltimore). 2017. PMID: 29390333 Free PMC article.
-
[A case of sclerosed hemangioma mimicking intrahepatic cholangiocarcinoma].Korean J Gastroenterol. 2009 Dec;54(6):399-403. doi: 10.4166/kjg.2009.54.6.399. Korean J Gastroenterol. 2009. PMID: 20026896 Korean.
-
Hepatic Sclerosed Hemangioma: a case report and review of the literature.BMC Surg. 2015 Apr 17;15:45. doi: 10.1186/s12893-015-0029-x. BMC Surg. 2015. PMID: 25927893 Free PMC article. Review.
-
Synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma: A case report and review of the literature.Medicine (Baltimore). 2021 Nov 19;100(46):e27349. doi: 10.1097/MD.0000000000027349. Medicine (Baltimore). 2021. PMID: 34797273 Free PMC article. Review.
-
Intrahepatic cholangiocarcinoma in liver hemangioma with hepatitis B infection.Dig Liver Dis. 2013 Nov;45(11):e14. doi: 10.1016/j.dld.2013.05.004. Epub 2013 Jun 21. Dig Liver Dis. 2013. PMID: 23791801 No abstract available.
References
-
- Nakano M, Ariizumi SI, Yamamoto M. Intrahepatic cholangiocarcinoma. Semin Diagn Pathol 2017;34:160–6. - PubMed
-
- Farges O, Fuks D, Le Treut YP, et al. AJCC 7th edition of TNM staging accurately discriminates outcomes of patients with resectable intrahepatic cholangiocarcinoma: by the AFC-IHCC-2009 study group. Cancer 2011;117:2170–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
