

Thyroid blood flow in inferior thyroid artery as predictor for increase in levothyroxine dosage during pregnancy in women with Hashimoto's thyroiditis - a retrospective study
- PMID: 31277608
- PMCID: PMC6612150
- DOI: 10.1186/s12884-019-2389-1
Thyroid blood flow in inferior thyroid artery as predictor for increase in levothyroxine dosage during pregnancy in women with Hashimoto's thyroiditis - a retrospective study
Abstract
Background: We examined whether inferior thyroid artery peak systolic velocity (ITA-PSV) predicts an increase in levothyroxine (LT4) dosage in pregnant women with Hashimoto's thyroiditis.
Methods: Twenty-two women with Hashimoto's thyroiditis who were planning and later achieved pregnancy or confirmed as pregnant were enrolled in this retrospective longitudinal observational study. ITA-PSV and thyroid volume were measured using ultrasonography. Serum concentrations of free thyroxine (F-T4), free triiodothyronine (F-T3), and thyroid stimulating hormone (TSH) were simultaneously determined. We adjusted LT4 dosage to maintain serum TSH at < 2.5 μIU/mL (1st trimester) and later at < 3 μIU/mL (2nd, 3rd trimester).
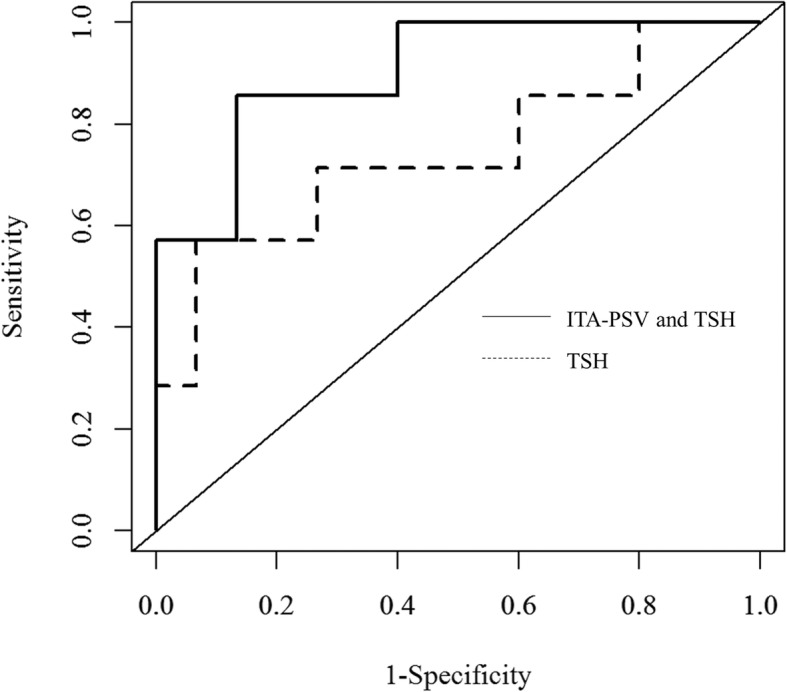
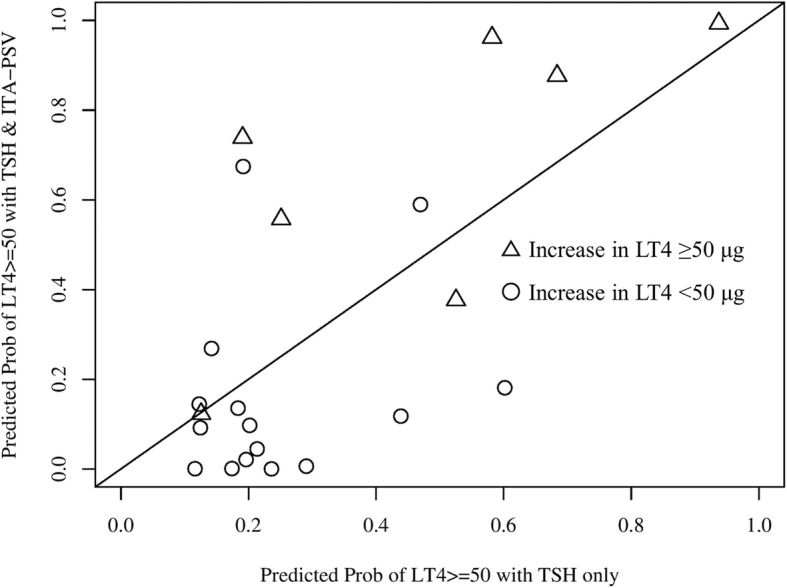
Results: Eighteen patients (81.8%) required an increase in LT4 dosage during pregnancy, of whom 7 (31.8%) required an increase ≥50 μg. Multivariable regression analysis showed that TSH (β = 0.507, p = 0.008) and ITA-PSV (β = - 0.362, p = 0.047), but not thyroid volume, F-T4, or F-T3, were independently associated with increased LT4 dosage. Receiver-operating characteristic analysis for predicting an increase in LT4 ≥ 50 μg/day showed that the area under the curve (0.905) for ITA-PSV with TSH was not significantly increased (p = 0.123) as compared to that (0.743) for TSH alone, whereas integrated discrimination improvement was significantly increased (27.9%, p = 0.009).
Conclusions: In pregnant patients with Hashimoto's thyroiditis, ITA-PSV was a significant predictor of increase in LT4 dosage independent of TSH level, while ITA-PSV plus TSH showed significantly improved predictability as compared to TSH alone. These results suggest that ITA-PSV reflects residual thyroid function and is useful for evaluating the need for increased thyroid hormone production in pregnant patients with Hashimoto's thyroiditis.
Keywords: Hashimoto’s thyroiditis; ITA-PSV; Levothyroxine dosage; Pregnancy.
Conflict of interest statement
The authors have no competing interests to declare.
Figures
Similar articles
-
Remission of Hashimoto's thyroiditis in a twelve-year-old girl with thyroid changes documented by ultrasonography.Thyroid. 2010 Oct;20(10):1187-90. doi: 10.1089/thy.2010.0102. Thyroid. 2010. PMID: 20883175
-
Impact of Laboratory-Measured Euthyroid Hashimoto's Thyroiditis on Reproductive Hormone Profile in Women with Obesity.Metab Syndr Relat Disord. 2025 May;23(4):211-216. doi: 10.1089/met.2024.0181. Epub 2024 Dec 10. Metab Syndr Relat Disord. 2025. PMID: 39655636
-
Compared with classic Hashimoto's thyroiditis, chronic autoimmune serum-negative thyroiditis requires a lower substitution dose of L-thyroxine to correct hypothyroidism.J Endocrinol Invest. 2020 Nov;43(11):1631-1636. doi: 10.1007/s40618-020-01249-x. Epub 2020 Apr 21. J Endocrinol Invest. 2020. PMID: 32319047
-
A meta-analysis: elucidating diagnostic thresholds of peak systolic flow velocities in thyroid arteries for the discrimination of Graves' disease and destructive thyrotoxicosis.Front Endocrinol (Lausanne). 2024 Jun 7;15:1393126. doi: 10.3389/fendo.2024.1393126. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38911037 Free PMC article. Review.
-
[Monitoring of treatment in thyroid diseases].Ther Umsch. 1999 Jul;56(7):400-2. doi: 10.1024/0040-5930.56.7.400. Ther Umsch. 1999. PMID: 10434779 Review. German.
Cited by
-
Quantitative Diagnosis Progress of Ultrasound Imaging Technology in Thyroid Diffuse Diseases.Diagnostics (Basel). 2023 Feb 13;13(4):700. doi: 10.3390/diagnostics13040700. Diagnostics (Basel). 2023. PMID: 36832188 Free PMC article. Review.
References
-
- Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, O'Heir CE, Mitchell ML, Hermos RJ, Waisbren SE, et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999;341(8):549–555. doi: 10.1056/NEJM199908193410801. - DOI - PubMed
-
- Leung AS, Millar LK, Koonings PP, Montoro M, Mestman JH. Perinatal outcome in hypothyroid pregnancies. Obstet Gynecol. 1993;81(3):349–353. - PubMed
-
- Stagnaro-Green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, Nixon A, Pearce EN, Soldin OP, Sullivan S, et al. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21(10):1081–1125. doi: 10.1089/thy.2011.0087. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
