

Kaposiform lymphangiomatosis and kaposiform hemangioendothelioma: similarities and differences
- PMID: 31277673
- PMCID: PMC6612206
- DOI: 10.1186/s13023-019-1147-9
Kaposiform lymphangiomatosis and kaposiform hemangioendothelioma: similarities and differences
Abstract
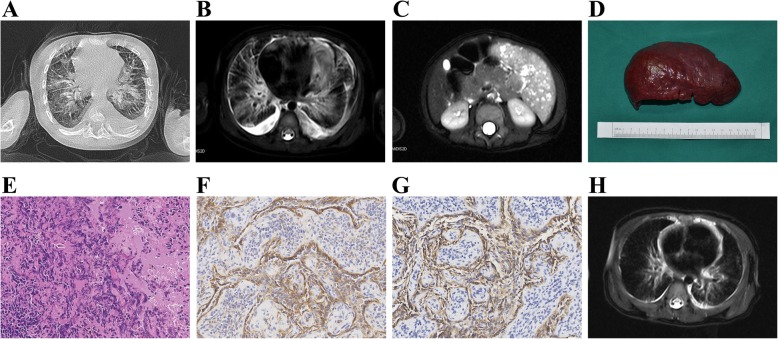
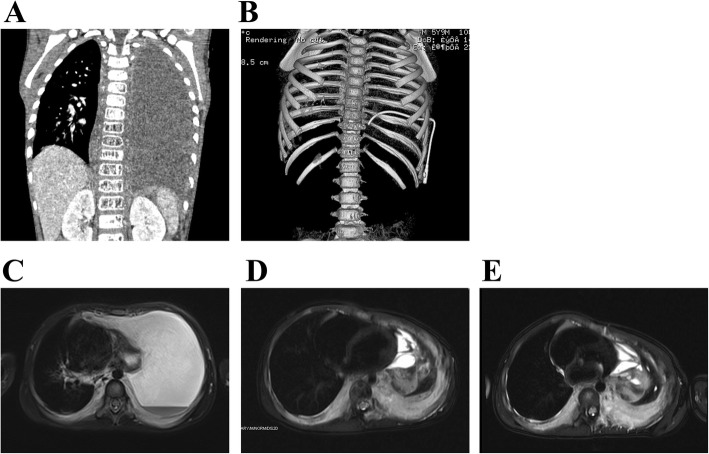
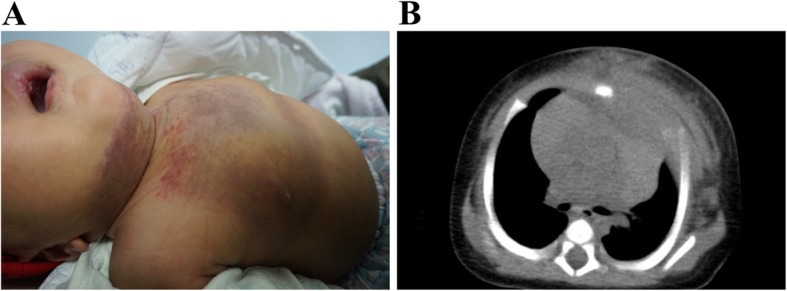
Background: Kaposiform lymphangiomatosis (KLA) and kaposiform hemangioendothelioma (KHE) are rare and aggressive vascular disorders. The aim of this study was to examine the clinical features and prognosis of KLA and KHE involving the thorax.
Methods: The clinical features, imaging and pathological findings, treatments and outcome were retrospectively reviewed for 6 patients with KLA and 7 patients with KHE involving the thorax.
Results: The mean ages at the time of the presentation of signs/symptoms were 26.7 months and 4.1 months for KLA and KHE, respectively. Respiratory symptoms, pericardial and pleural effusion, thrombocytopenia and coagulopathy were common in both KLA and KHE. Diffuse lesions involving the lung and extrathoracic sites were observed in KLA but not in KHE. Histopathologically, all lesions had spindled tumor cells, which were immunoreactive for CD31 and D2-40. In KLA, the spindle cells were distributed in sparse and poorly marginated clusters, whereas the spindle cells formed more defined and confluent vascularized nodules in KHE. Unlike the refractory behavior of KLA, the majority of patients with KHE responded to medical treatments with regression of the lesion and normalization of the hematologic parameters.
Conclusions: The presenting and histological characteristics of KLA can overlap with those of KHE. The presence of diffuse vascular lesions in the mediastinum and lung with refractory thrombocytopenia and coagulopathy should suggest the diagnosis of KLA. Given the rarity and high morbidity and mortality of these disorders, the diagnostic process and therapeutic approach should include a multidisciplinary team review and consensus.
Keywords: Coagulopathy; Kaposiform hemangioendothelioma; Kaposiform lymphangiomatosis; Thorax; Thrombocytopenia.
Conflict of interest statement
The authors declare that they have no competing interests, either financial or non-financial, that could be perceived as prejudicing the impartiality of the research reported.
Figures

References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
