

Acceptance and Commitment Therapy to Increase Adherence to Penile Injection Therapy-Based Rehabilitation After Radical Prostatectomy: Pilot Randomized Controlled Trial
- PMID: 31277968
- PMCID: PMC6943977
- DOI: 10.1016/j.jsxm.2019.05.013
Acceptance and Commitment Therapy to Increase Adherence to Penile Injection Therapy-Based Rehabilitation After Radical Prostatectomy: Pilot Randomized Controlled Trial
Abstract
Introduction: Despite the importance of using penile injections as part of a penile rehabilitation program, men have difficulty complying with these programs.
Aim: To test a novel psychological intervention based on Acceptance and Commitment Therapy for erectile dysfunction (ACT-ED) to help men utilize penile injections.
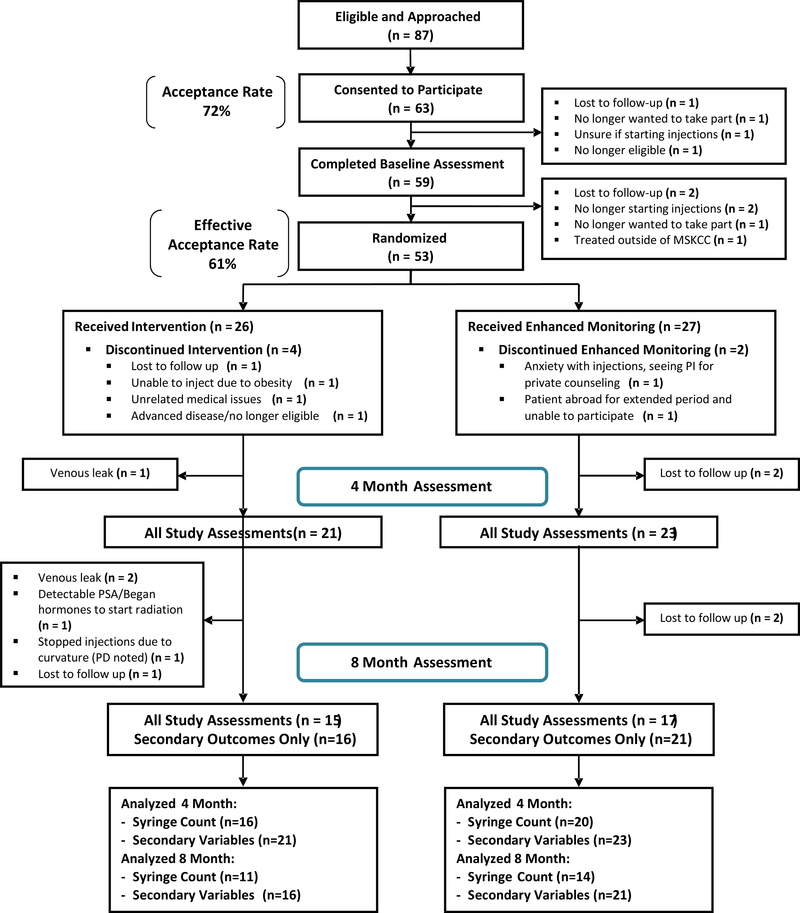
Methods: This pilot randomized controlled trial (RCT) recruited men who were beginning a standard care (SC) structured penile rehabilitation program following radical prostatectomy. The SC program instructed patients to use penile injections 2 to 3 times per week. Participants were randomized to SC+ACT-ED or SC+enhanced monitoring (EM). Over 4 months, patients in the SC+ACT-ED group received SC plus 4 ACT sessions and 3 ACT phone calls; those in the EM group received SC plus 7 phone calls from an experienced sexual medicine nurse practitioner. Participants were assessed at study entry and at 4 and 8 months. For this pilot study, the goal was to determine initial efficacy (ie, effect sizes, where d = 0.2 is small, d = 0.5 is medium, and d = 0.8 is large).
Main outcome measure: Primary outcomes were feasibility and use of penile injections. Secondary outcomes were ED treatment satisfaction (ie, Erectile Dysfunction Inventory of Treatment Satisfaction, or EDITS), sexual Self-Esteem and Relationship (SEAR) quality, sexual bother (SB), and prostate cancer treatment regret.
Results: The 53 participants were randomized (ACT, n = 26; EM, n = 27). The study acceptance rate was 61%. At 4 months, the ACT-ED group utilized more penile injections per week (1.7) compared to the EM group (0.9) (d = 1.25; P = .001) and was more adherent to penile rehabilitation compared to the EM group (ACT, 44%; EM, 10%; relative risk [RR], 4.4; P = .02). These gains were maintained at 8 months for injections per week (ACT, 1.2; EM, 0.7; d = 1.08; P = .03) and approached significance for adherence (ACT, 18%; EM, 0%; P = .10). At 4 months, ACT-ED, compared to EM, reported moderate effects for greater satisfaction with ED treatment (d = 0.41; P = .22), greater sexual self-esteem (d = 0.54; P = .07) and sexual confidence (d = 0.48; P = .07), lower sexual bother (d = 0.43; P = .17), and lower prostate cancer treatment regret (d = 0.74; P = .02). At 8 months, moderate effects in favor of ACT-ED were maintained for greater sexual self-esteem (d = 0.40; P = .19) and less treatment regret (d = 0.47; P = .16).
Clinical implications: ACT concepts may help men utilize penile injections and cope with the effects of ED.
Strengths and limitations: Strengths include use of an innovative intervention utilizing ACT concepts and pilot RCT. Limitations include the pilot nature of the study (eg, small samples size, lack of statistical power).
Conclusion: ACT-ED is feasible and significantly increases the use of penile injections. ACT-ED also shows promise (moderate effects) for increasing satisfaction with penile injections and sexual self-esteem while decreasing sexual bother and prostate cancer treatment regret. Nelson CJ, Saracino RM, Napolitano S, et al. Acceptance and Commitment Therapy to Increase Adherence to Penile Injection Therapy-Based Rehabilitation After Radical Prostatectomy: Pilot Randomized Controlled Trial. J Sex Med 2019; 19:1398-1408.
Keywords: Erectile Dysfunction; Erectile Rehabilitation; Prostate Cancer; Sexual Function.
Copyright © 2019 International Society for Sexual Medicine. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Erectile rehabilitation with intracavernous alprostadil after radical prostatectomy: refusal and dropout rates.BJU Int. 2012 Dec;110(11 Pt C):E954-7. doi: 10.1111/j.1464-410X.2012.11484.x. Epub 2012 Oct 19. BJU Int. 2012. PMID: 23078100
-
Quality of Life, Psychological Functioning, and Treatment Satisfaction of Men Who Have Undergone Penile Prosthesis Surgery Following Robot-Assisted Radical Prostatectomy.J Sex Med. 2017 Dec;14(12):1612-1620. doi: 10.1016/j.jsxm.2017.10.001. Epub 2017 Oct 27. J Sex Med. 2017. PMID: 29111200
-
Penile Rehabilitation Therapy Following Radical Prostatectomy: A Meta-Analysis.J Sex Med. 2017 Dec;14(12):1496-1503. doi: 10.1016/j.jsxm.2017.09.020. Epub 2017 Nov 6. J Sex Med. 2017. PMID: 29122494 Review.
-
The Role of the Low-Intensity Extracorporeal Shockwave Therapy on Penile Rehabilitation After Radical Prostatectomy: A Randomized Clinical Trial.J Sex Med. 2020 Apr;17(4):688-694. doi: 10.1016/j.jsxm.2019.12.024. Epub 2020 Jan 30. J Sex Med. 2020. PMID: 32007430 Clinical Trial.
-
Penile rehabilitation for postprostatectomy erectile dysfunction.Cochrane Database Syst Rev. 2018 Oct 23;10(10):CD012414. doi: 10.1002/14651858.CD012414.pub2. Cochrane Database Syst Rev. 2018. PMID: 30352488 Free PMC article.
Cited by
-
A contemporary review of the treatments and challenges associated with penile rehabilitation after radical prostatectomy including a proposed optimal approach.Int J Impot Res. 2024 Aug;36(5):480-485. doi: 10.1038/s41443-023-00782-6. Epub 2023 Oct 18. Int J Impot Res. 2024. PMID: 37853240 Review.
-
Current management strategy of treating patients with erectile dysfunction after radical prostatectomy: a systematic review and meta-analysis.Int J Impot Res. 2022 Jan;34(1):18-36. doi: 10.1038/s41443-020-00364-w. Epub 2020 Oct 24. Int J Impot Res. 2022. PMID: 33099581
-
Does sexual rehabilitation work for gay and bisexual prostate cancer patients? Acceptability, feasibility, and efficacy results from the Restore-2 randomized controlled trial.J Cancer Surviv. 2024 Sep 12. doi: 10.1007/s11764-024-01672-6. Online ahead of print. J Cancer Surviv. 2024. PMID: 39266938
-
Use of erectile dysfunction treatments after prostate cancer treatment and their perceived impact on men's sex life: an analysis of patient reported outcome survey data.BMC Urol. 2025 Jan 31;25(1):21. doi: 10.1186/s12894-025-01702-0. BMC Urol. 2025. PMID: 39891173 Free PMC article.
-
Mindfulness-based interventions for medication adherence: A systematic review and narrative synthesis.J Psychosom Res. 2021 Oct;149:110585. doi: 10.1016/j.jpsychores.2021.110585. Epub 2021 Jul 26. J Psychosom Res. 2021. PMID: 34332271 Free PMC article.
References
-
- ACS. Cancer Facts and Figures 2018. Atlanta: American Cancer Society; 2018.
-
- Nelson CJ, Deveci S, Stasi J, Scardino PT, Mulhall JP. Sexual bother following radical prostatectomyjsm. J Sex Med. 2010;7(1 Pt 1):129–35. - PubMed
-
- Liu Q, Zhang Y, Wang J, Li S, Cheng Y, Guo J, et al. Erectile Dysfunction and Depression: A Systematic Review and Meta-Analysis. J Sex Med. 2018;15(8):1073–82. - PubMed
