

A Pilot Randomized Trial of Ferric Citrate Coordination Complex for the Treatment of Advanced CKD
- PMID: 31278194
- PMCID: PMC6683712
- DOI: 10.1681/ASN.2018101016
A Pilot Randomized Trial of Ferric Citrate Coordination Complex for the Treatment of Advanced CKD
Abstract
Background: Researchers have yet to determine the optimal care of patients with advanced CKD. Evidence suggests that anemia and CKD-related disordered mineral metabolism (including abnormalities in phosphate and fibroblast growth factor 23 [FGF23]) contribute to adverse outcomes in this population.
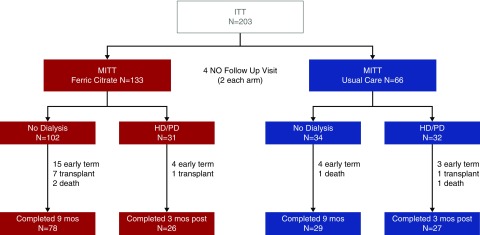
Methods: To investigate whether fixed-dose ferric citrate coordination complex favorably affects multiple biochemical parameters in patients with advanced CKD, we randomly assigned 203 patients with eGFR≤20 ml/min per 1.73 m2 2:1 to receive a fixed dose of ferric citrate coordination complex (two tablets per meal, 210 mg ferric iron per tablet) or usual care for 9 months or until 3 months after starting dialysis. No single biochemical end point was designated as primary; sample size was determined empirically.
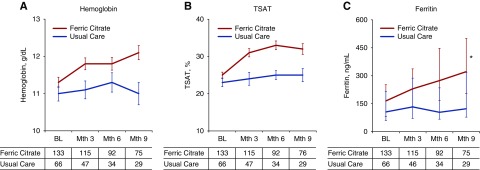
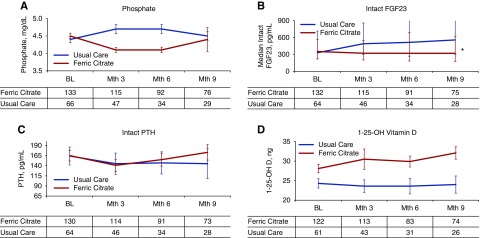
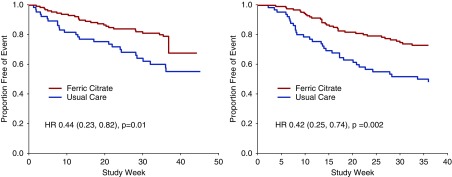
Results: The two groups had generally similar baseline characteristics, although diabetes and peripheral vascular disease were more common in the usual-care group. Ferric citrate coordination complex significantly increased hemoglobin, transferrin saturation, and serum ferritin, and it significantly reduced serum phosphate and intact FGF23 (P<0.001 for all). Of the 133 patients randomized to ferric citrate coordination complex, 31 (23%) initiated dialysis during the study period, as did 32 of 66 (48%) patients randomized to usual care (P=0.001). Compared with usual care, ferric citrate coordination complex treatment resulted in significantly fewer annualized hospital admissions, fewer days in hospital, and a lower incidence of the composite end point of death, provision of dialysis, or transplantation (P=0.002).
Conclusions: The beneficial effects of fixed-dose ferric citrate coordination complex on biochemical parameters, as well as the exploratory results regarding the composite end point and hospitalization, suggest that fixed-dose ferric citrate coordination complex has an excellent safety profile in an unselected population with advanced CKD and merits further study.
Keywords: CKD; FGF23; RCT; anemia; ferric citrate; hyperphosphatemia.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group : KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl 76: 279–335, 2012
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group : KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl 2(4): S1–S140, 2009 - PubMed
-
- Besarab A, Bolton WK, Browne JK, Egrie JC, Nissenson AR, Okamoto DM, et al. .: The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med 339: 584–590, 1998 - PubMed
-
- Drüeke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall IC, Tsakiris D, et al. .: CREATE Investigators : Normalization of hemoglobin level in patients with chronic kidney disease and anemia. N Engl J Med 355: 2071–2084, 2006 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
