

British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma
- PMID: 31278206
- PMCID: PMC6709778
- DOI: 10.1136/gutjnl-2018-318126
British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma
Abstract
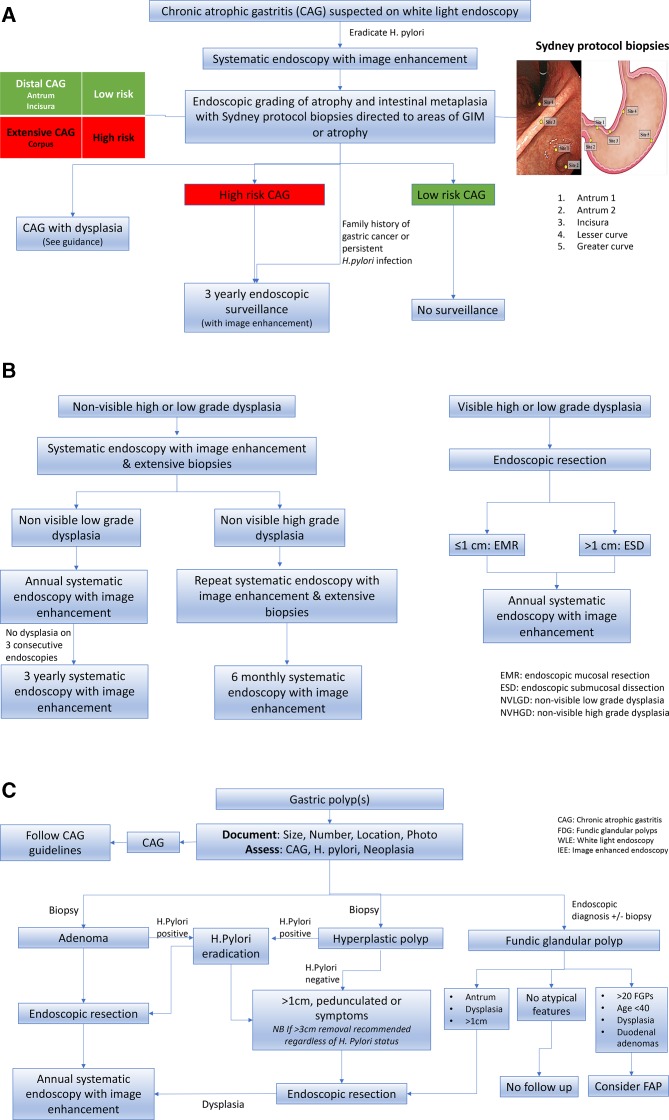
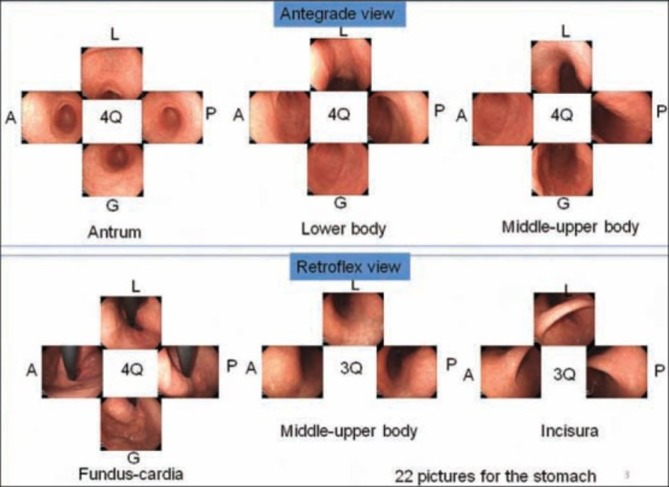
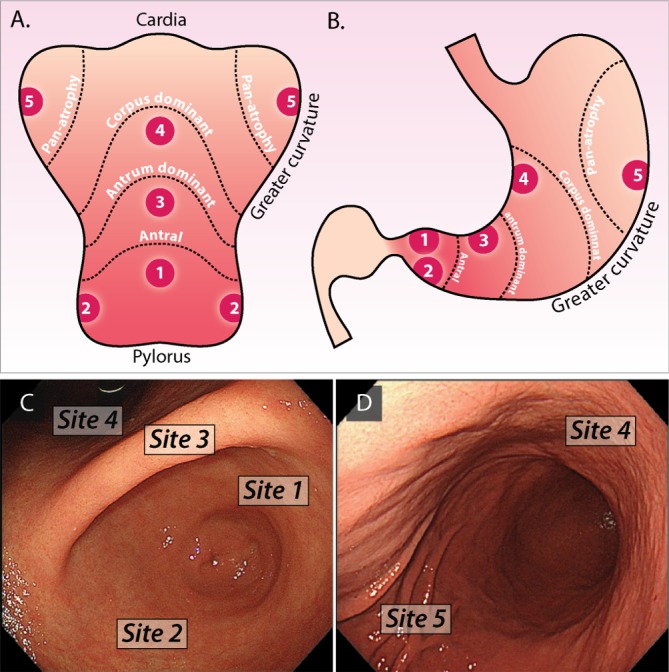
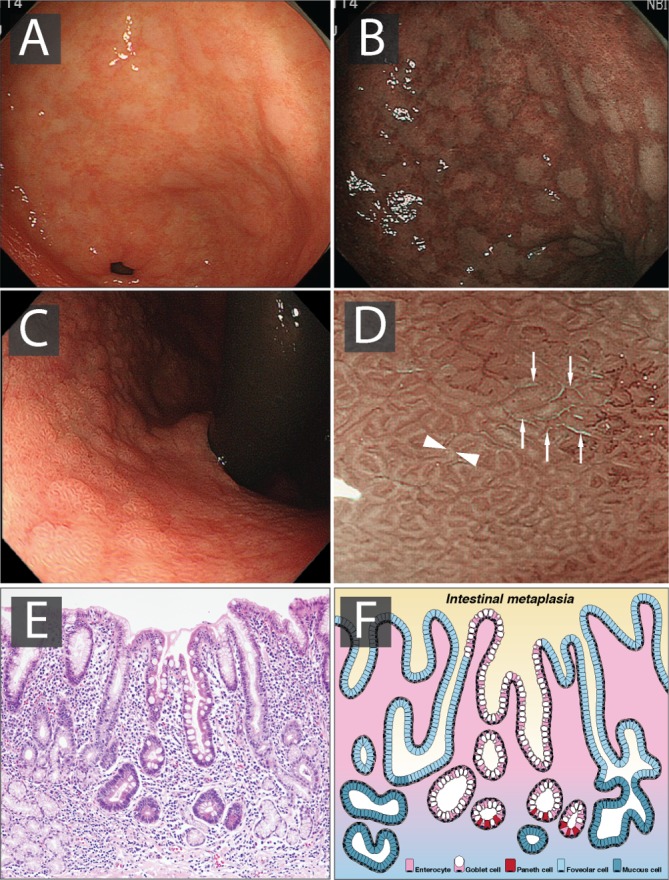
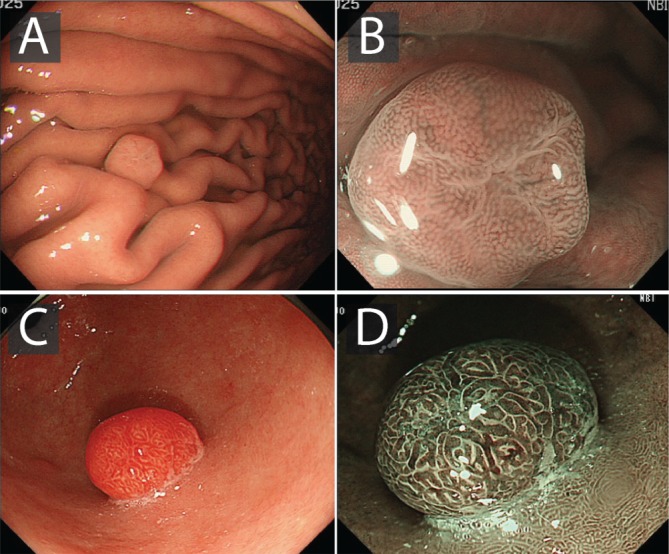
Gastric adenocarcinoma carries a poor prognosis, in part due to the late stage of diagnosis. Risk factors include Helicobacter pylori infection, family history of gastric cancer-in particular, hereditary diffuse gastric cancer and pernicious anaemia. The stages in the progression to cancer include chronic gastritis, gastric atrophy (GA), gastric intestinal metaplasia (GIM) and dysplasia. The key to early detection of cancer and improved survival is to non-invasively identify those at risk before endoscopy. However, although biomarkers may help in the detection of patients with chronic atrophic gastritis, there is insufficient evidence to support their use for population screening. High-quality endoscopy with full mucosal visualisation is an important part of improving early detection. Image-enhanced endoscopy combined with biopsy sampling for histopathology is the best approach to detect and accurately risk-stratify GA and GIM. Biopsies following the Sydney protocol from the antrum, incisura, lesser and greater curvature allow both diagnostic confirmation and risk stratification for progression to cancer. Ideally biopsies should be directed to areas of GA or GIM visualised by high-quality endoscopy. There is insufficient evidence to support screening in a low-risk population (undergoing routine diagnostic oesophagogastroduodenoscopy) such as the UK, but endoscopic surveillance every 3 years should be offered to patients with extensive GA or GIM. Endoscopic mucosal resection or endoscopic submucosal dissection of visible gastric dysplasia and early cancer has been shown to be efficacious with a high success rate and low rate of recurrence, providing that specific quality criteria are met.
Keywords: endoscopy; gastric adenocarcinoma; gastric pre-cancer; gastritis; helicobacter pylori-gastritis.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
There is much more to rely on histology than the sole endoscopy tells us.Gut. 2020 Sep;69(9):1. doi: 10.1136/gutjnl-2019-319649. Epub 2019 Aug 31. Gut. 2020. PMID: 31473597 No abstract available.
-
ESD, not EMR, should be the first-line therapy for early gastric neoplasia.Gut. 2020 Sep;69(9):1-2. doi: 10.1136/gutjnl-2019-319646. Epub 2019 Sep 3. Gut. 2020. PMID: 31481547 No abstract available.
-
EMR achieves similar oncological outcomes as ESD for gastric neoplasia of <1cm, requiring less expertise, training and time.Gut. 2020 Sep;69(9):1. doi: 10.1136/gutjnl-2019-319925. Epub 2019 Oct 5. Gut. 2020. PMID: 31586933 No abstract available.
-
Early detection and risk stratification of gastric cancer are likely to be refined with biopsies targeted through high-resolution-enhanced imaging.Gut. 2020 Sep;69(9):1. doi: 10.1136/gutjnl-2019-319921. Epub 2019 Oct 14. Gut. 2020. PMID: 31611299 No abstract available.
-
Gastric biopsies in the assessment and management of patients at risk of gastric adenocarcinoma.Gut. 2021 Feb;70(2):431-432. doi: 10.1136/gutjnl-2020-321053. Epub 2020 May 23. Gut. 2021. PMID: 32447310 No abstract available.
-
Prevalence of gastric intestinal metaplasia in a single-centre multicultural Australian cohort.Intern Med J. 2023 Feb;53(2):296-297. doi: 10.1111/imj.16010. Intern Med J. 2023. PMID: 36822609 No abstract available.
References
-
- Cancer Research UK. Stomach cancer statistics | Cancer Research UK [Internet]. 2016. http://www.cancerresearchuk.org/health-professional/cancer-statistics/st... (cited 14 Mar 2018).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous