

Comparing socioeconomic inequalities between early neonatal mortality and facility delivery: Cross-sectional data from 72 low- and middle-income countries
- PMID: 31278283
- PMCID: PMC6611781
- DOI: 10.1038/s41598-019-45148-5
Comparing socioeconomic inequalities between early neonatal mortality and facility delivery: Cross-sectional data from 72 low- and middle-income countries
Abstract
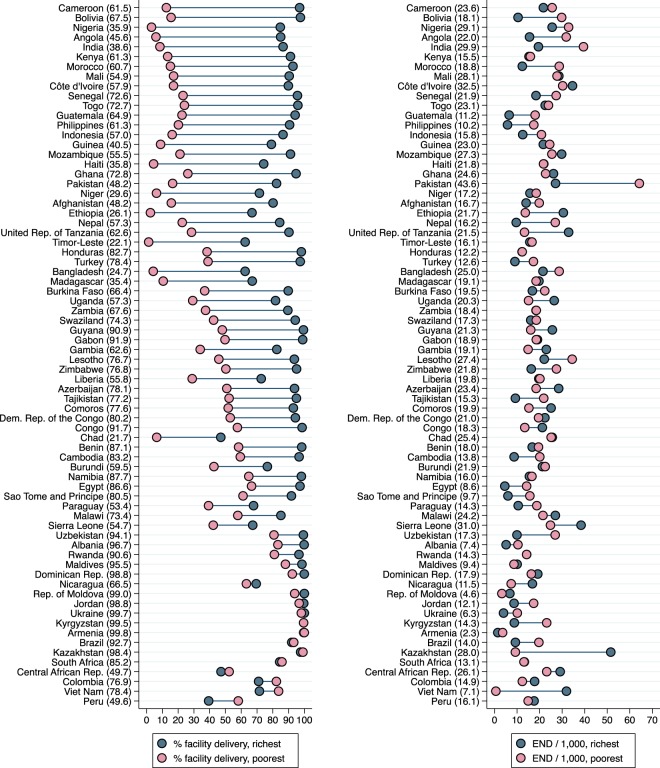
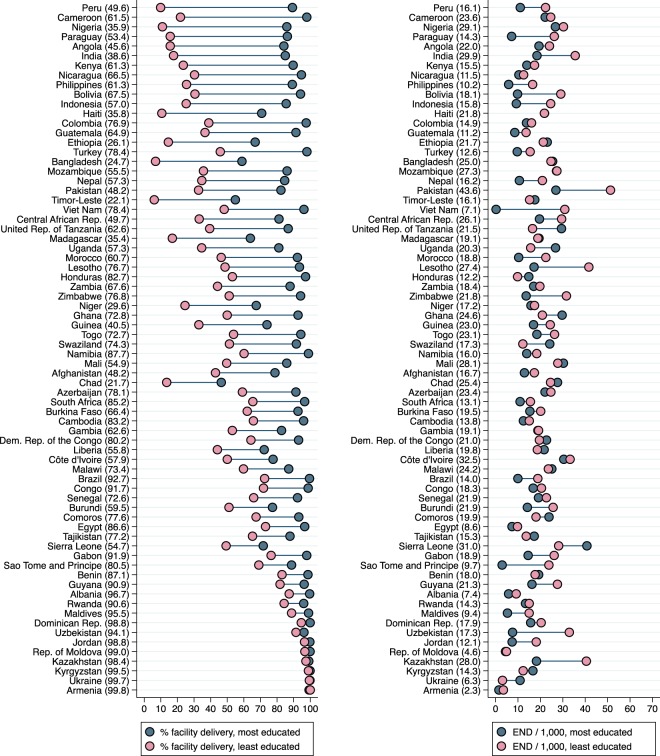
Facility delivery should reduce early neonatal mortality. We used the Slope Index of Inequality and logistic regression to quantify absolute and relative socioeconomic inequalities in early neonatal mortality (0 to 6 days) and facility delivery among 679,818 live births from 72 countries with Demographic and Health Surveys. The inequalities in early neonatal mortality were compared with inequalities in postneonatal infant mortality (28 days to 1 year), which is not related to childbirth. Newborns of the richest mothers had a small survival advantage over the poorest in unadjusted analyses (-2.9 deaths/1,000; OR 0.86) and the most educated had a small survival advantage over the least educated (-3.9 deaths/1,000; OR 0.77), while inequalities in postneonatal infant mortality were more than double that in absolute terms. The proportion of births in health facilities was an absolute 43% higher among the richest and 37% higher among the most educated compared to the poorest and least educated mothers. A higher proportion of facility delivery in the sampling cluster (e.g. village) was only associated with a small decrease in early neonatal mortality. In conclusion, while socioeconomically advantaged mothers had much higher use of a health facility at birth, this did not appear to convey a comparable survival advantage.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- WHO. Global Health Observatory (GHO) data. Neonatal mortality. Situation and trends. https://who.int/gho/child-health/mortality/neonatal_text/en/ (2019).
-
- Wang H, Bhutta ZA, Coates MM, Coggeshall M. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1725–1774. doi: 10.1016/S0140-6736(16)31575-6. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
